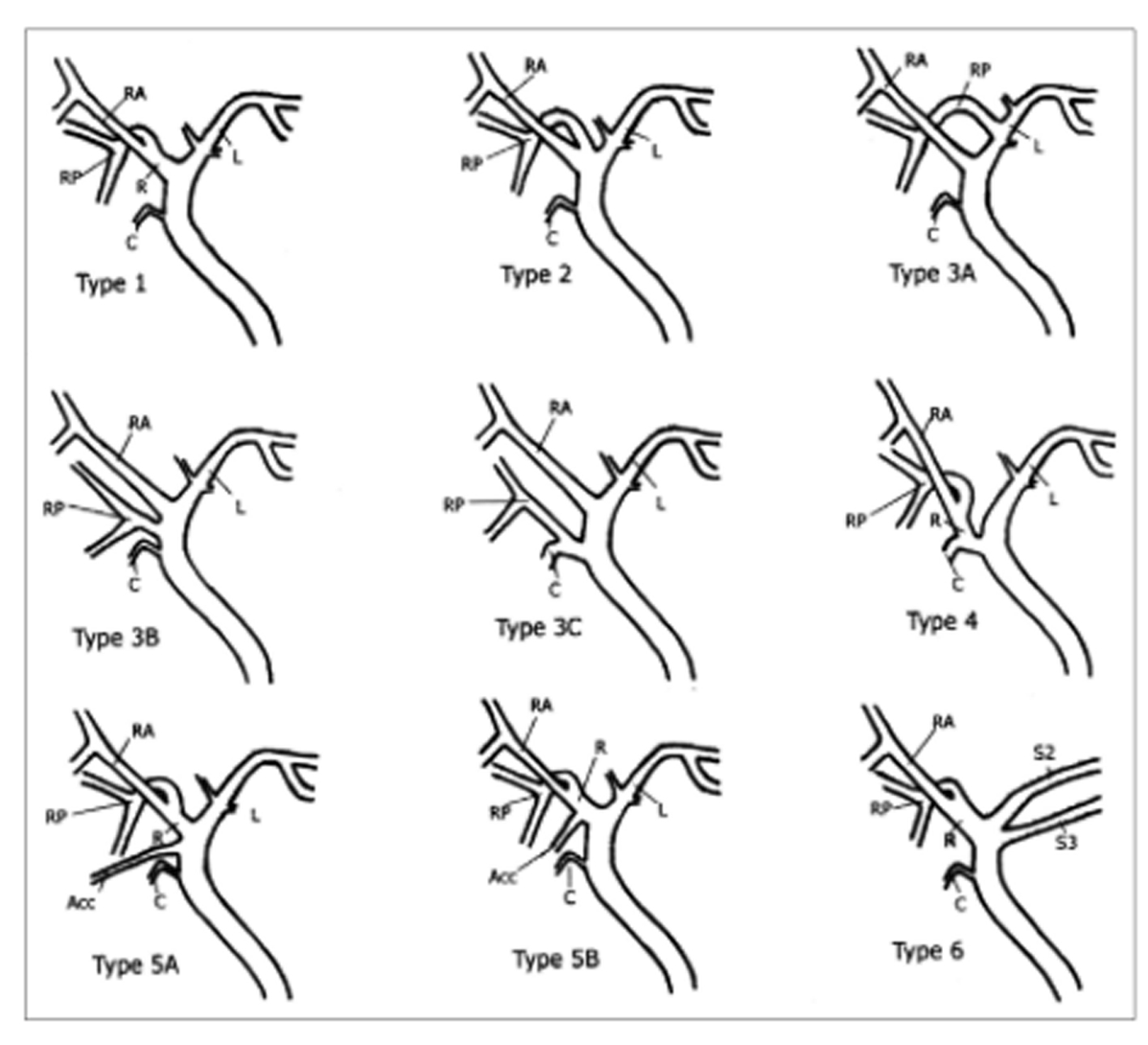
Figure 1. Schematic drawing of IHD anatomy. Type 1 is typical. Type 2 involves triple confluence, the simultaneous emptying of the RASD, RPSD and LHD into the CHD. In type 3, the RPSD drains anomalously, and in type 4, the RHD drains into the cystic duct. In type 5, an accessory duct is present, and in type 6, segments II and III drain individually into the RHD or CHD. Type 7 shows unclassified or complex variation. R: right hepatic duct; L: left hepatic duct; RA: right anterior segmental duct; RP: right posterior segmental duct; C: cystic duct; Acc: accessory duct [7].