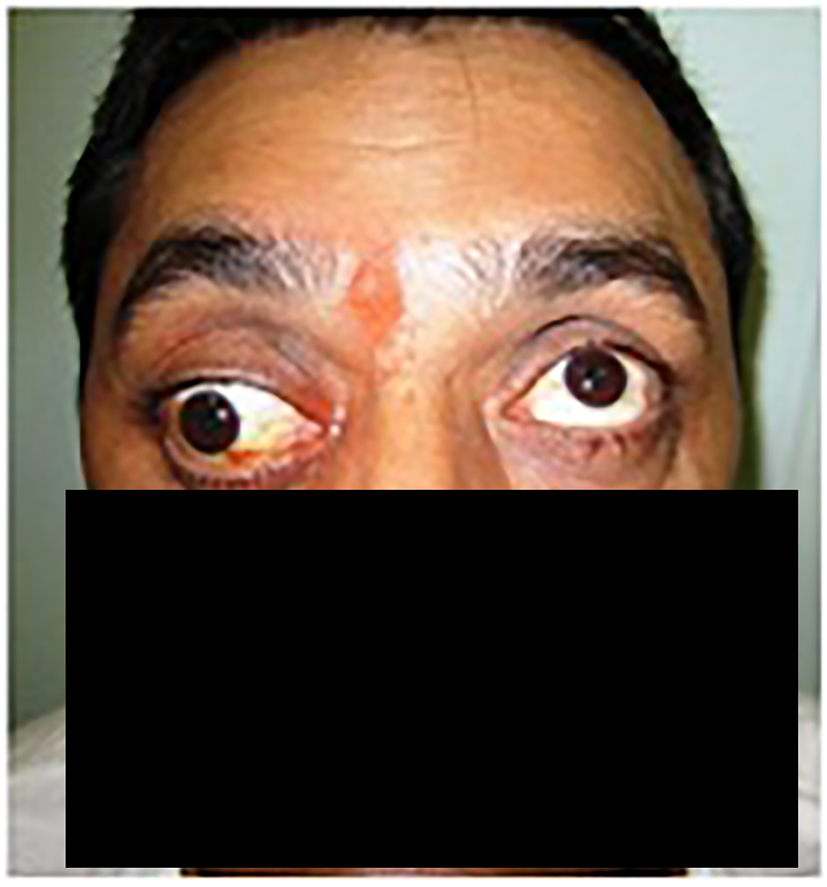
Figure 1. Proptosis of right eye and fixed eyeball seen when the patient came to OPD, with dilated pupil. This finding was correlating with poor vision of the patient from the same eye.
| Journal of Current Surgery, ISSN 1927-1298 print, 1927-1301 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Curr Surg and Elmer Press Inc |
| Journal website http://www.currentsurgery.org |
Case Report
Volume 6, Number 2, June 2016, pages 60-64
Fronto-Temporo-Zygomatic Approach for Orbital Apex and Infratemporal Fossa
Figures


Table
| Name | Approach | Lesions |
|---|---|---|
| Pellerin et al | Orbito-fronto-mallar approach | Orbital meningioma |
| Hakuba et al | Orbito-zygomatic ITF approach Fronto-orbito-temporal craniotomy. Three separate bone flaps | Cavernous sinus lesions |
| Frazier | Concept of removing orbital rims | Improved exposure of skull base |
| Delashaw et al | Fronto-temporal flap + superior and lateral orbital rim + frontal sinus. Zygomatic arch removed separately | Anterior fossa, middle fossa, orbit, cavernous sinus |
| McDermott | Removal of fronto-temporal and orbito-zygomatic bone flaps separately | |
| Al Mefty | Incorporated superior orbital ridges with pterional craniotomy | |
| Morwani et al | Modified fronto-temporo-zygomatic approach | Limited disease in ITF, lateral orbit and orbital apex |