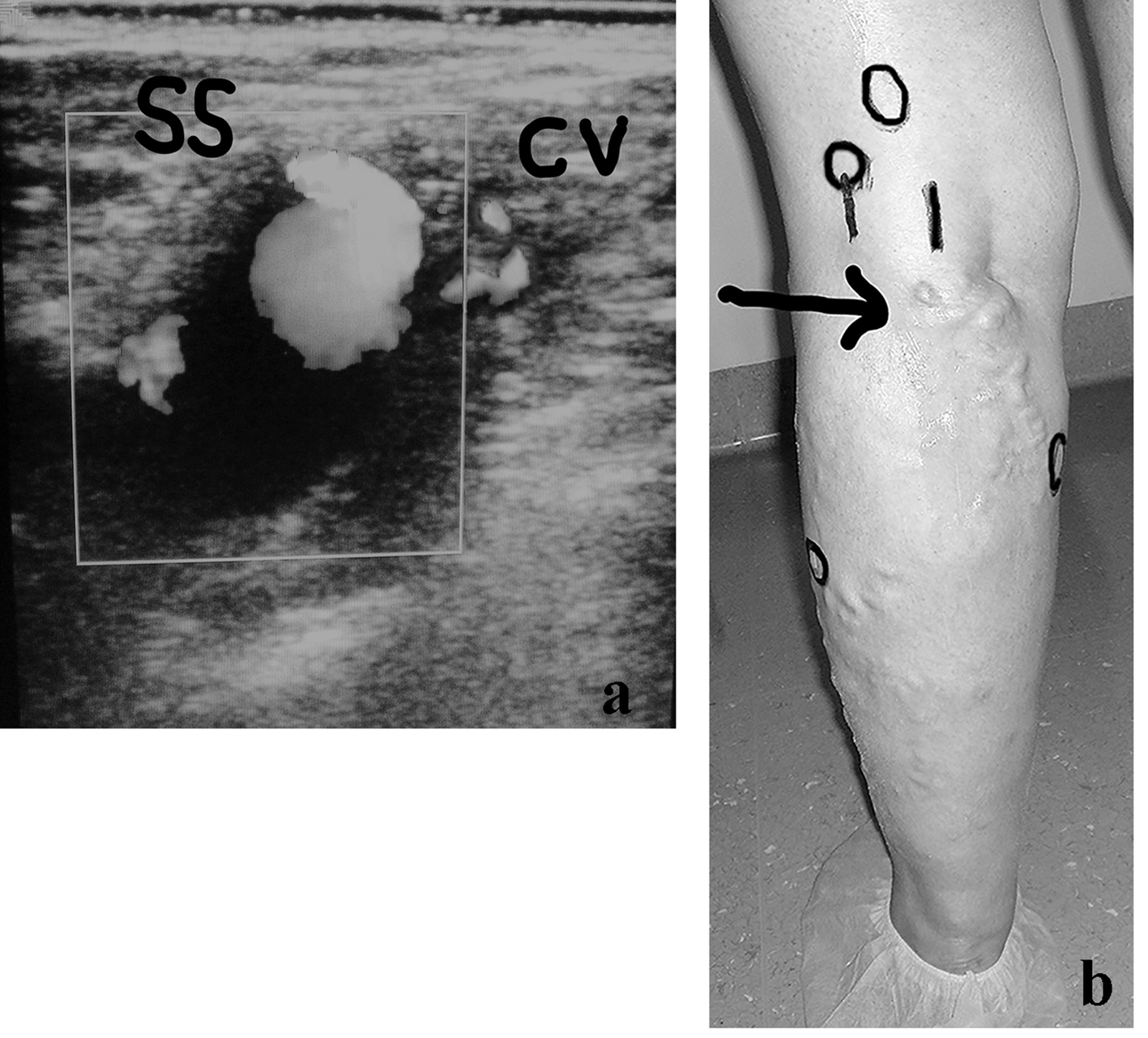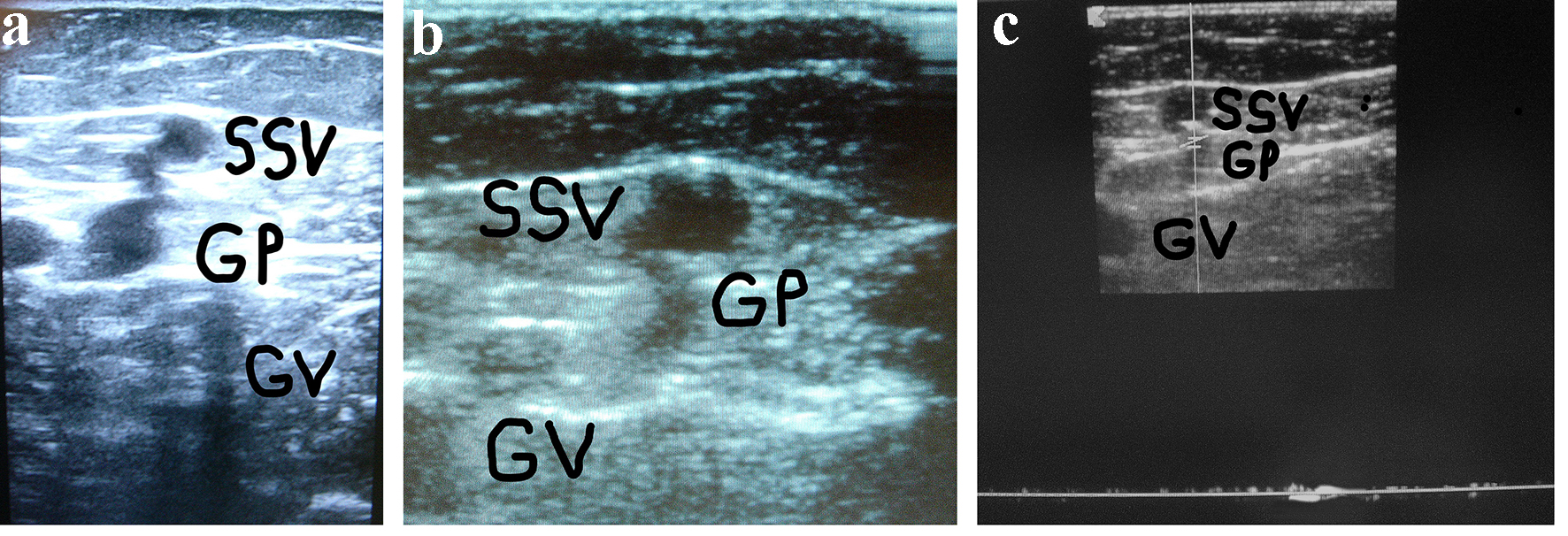
Figure 1. (a) A woman of 67 years of age. Appearance of symptomatic VR in the PR 4 years after the previous surgical procedure for varicose veins at the PR. Cross scanning of DUS examination at the PR: incompetent gastrocnemius perforator (GP) connected with the long residual SSV stump. The internal gastrocnemius vein (GV) is visible. (b) Treatment: SPJ surgical interruption and intraoperative DUS-guided foam sclerotherapy of gastrocnemius perforator (GP) and residual SSV. DUS examination after 30 days: the SS stump is not compressible and partially hyper-echogenic from early fibrosis (SSV), the gastrocnemius perforator (GP) is hyper-echogenic from early complete fibrosis in the subfascial segment, the internal gastrocnemius vein (GV) is patent and compressible. (c) DUS examination after 30 days: the gastrocnemius perforator (GP) is occluded with no flow into the lumen, the SS stump is not compressible and hyper-echogenic from advanced fibrosis (SSV), the internal gastrocnemius vein (GV) is patent and compressible.