

| Journal of Current Surgery, ISSN 1927-1298 print, 1927-1301 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Curr Surg and Elmer Press Inc |
| Journal website http://www.currentsurgery.org |
Case Report
Volume 4, Number 2, June 2014, pages 55-57
Transmesocolic Hernia Without a History of Digestive Surgery: Unknown Disease
Radwan Kassira, d, Claire Boutetb, Pierre Blancc, Olivier Tiffeta
aDepartment of General Surgery, CHU Hospital, Jean Monnet University, Saint Etienne, France
bDepartment of Radiology, CHU Hospital, Jean Monnet University, Saint Etienne, France
cDepartment of General Surgery, Clinique Chirurgicale Mutualiste, Saint Etienne, France
dCorresponding author: Radwan Kassir, Department of General Surgery, CHU Hospital, Jean Monnet University, Avenue Albert Raimond, 42270 Saint Etienne, France
Manuscript accepted for publication April 14, 2013
Short title: Transmesocolic Hernia
doi: https://doi.org/10.14740/jcs227w
| Abstract | ▴Top |
The incidence of internal hernia is less than 1%. Transmesocolic hernia (TH) is a rare type of internal hernia and it poses a real diagnostic challenge clinically. TH in patient without a history of operation hernia is an extremely rare phenomenon and is frequently none diagnosed. We report a case of TH in an adult patient without any preoperative history of digestive surgery. A 44-year-old woman was admitted to hospital for non-specific abdominal distension. The diagnosis of TH was suggested by computed tomography (CT). Entero-MRI confirmed the diagnostic. The symptoms were managed with conservative measures. The patient had no further pain during his follow-up and gave no recurrence. In the adult population, the cause of TH is previous gastrointestinal operation, intraperitoneal inflammation or trauma. Clinically, internal hernias can be asymptomatic, or can cause chronic dyspepsia, vague epigastric pain, intermittent colicky periumbilical pain, nausea and vomiting. There is extreme difficulty in making diagnosis of internal hernia preoperatively and the most important diagnostic method is abdominal CT and entero-MRI. This article illustrates the various types of internal hernias and imaging findings of TH. Even in cases with no previous laparotomy, it is important to consider the possibility of TH. We believe that conservative measures of TH are recommended in selected cases.
Keywords: Transmesocolic hernia; Small bowel obstruction; Internal hernia abdominal pain; CT scan; Conservative measures
| Introduction | ▴Top |
The incidence of internal hernia is less than 1% [1]. Internal hernia is a rare cause of small bowel obstruction, and transmesocolic hernia (TH) is a rare type of internal hernia and it poses a real diagnostic challenge clinically. THs are most often caused by previous surgical procedures (especially gastric bypass procedures), trauma or intraperitoneal inflammation. A review of the literature confirms that TH without a surgical history is extremely rare. An early diagnosis and treatment are required.
| Case Report | ▴Top |
We report an extremely rare case of TH in patient without a history of operation. A 44-year-old woman was admitted to hospital for chronic intermittent abdominal pain and bloating. She had no personal surgical history (except a hysterectomy) or trauma. Upon physical examination, the patient had non-specific abdominal distension. Laboratory assessment on admission was normal. Contrast-enhanced abdominal computed tomography (CT) and entero-MRI confirmed the presence of TH (Fig. 1). She was diagnosed as TH without surgical exploration. The symptoms were managed with conservative measures. The patient had no further pain during his follow-up and gave no recurrence. The period of follow-up is 10 months.
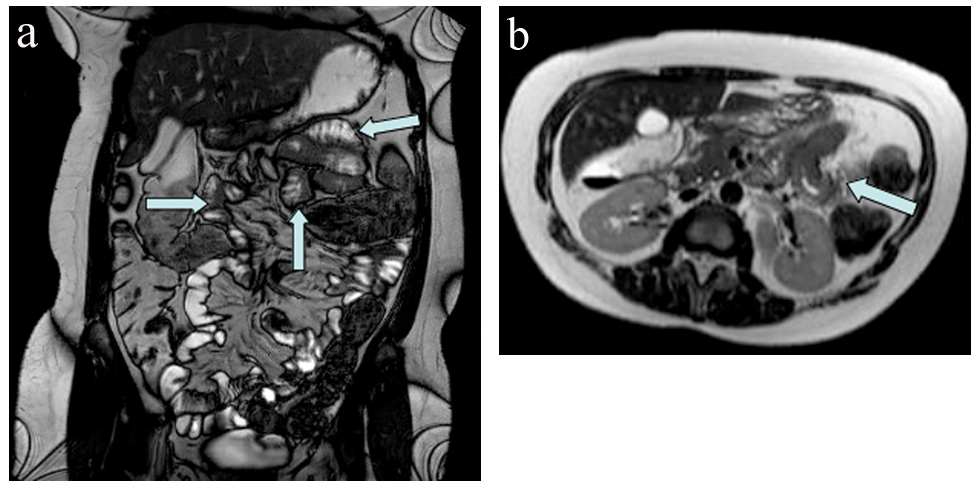 Click for large image | Figure 1. (a, b) Entero-MRI revealed a mildly dilated small bowel loops and a herniated sac through the transverse mesocolon (arrow). |
| Discussion | ▴Top |
Internal hernia is defined as the protrusion of one or more abdominal viscera through an anatomic or pathologic openings remaining inside the peritoneal cavity. Internal hernias account for approximately 0.5-5% of all cases of intestinal obstruction. Described by Meyers (Table 1), there are several main types based on their location: foramen of Winslow, ileocecal fossa, paraduodenal fossa, transmesentric, intersigmoid, the broad ligament of the uterus and retroanastomotic. The transmesenteric hernia has three main types: through a small-bowel mesenteric defect, transmesocolic and Peterson’s hernia. These hernias may be either congenital or acquired. Associated with a high mortality rate, most of the internal hernias are incidentally detected during surgical procedure (laparotomy and laparoscopy) or autopsy. The incidence of internal hernias is increasing because of new surgical procedures.
 Click to view | Table 1. Types of Internal Hernia |
TH is the rarest type of internal hernia (< 1%) and the more likely to develop a complication. TH was first reported by Rokitansky in 1836 [2]. TH is defined as internal hernia with a herniated sac through the transverse mesocolon. A subtype of internal hernia, TH has been extremely rarely described in the literature. The literature on TH published during last decade emphasizes that most of reported cases were associated with a history of surgical procedure or trauma, or congenital anormaly. The 35% of TH are observed among pediatric patients [3]. In our case, the patient was 44 years old. The most frequently complications of TH are: ischemia (40%) and volvulus (30%). TH can be rapidly lethal: the mortality rate for treated groups is more than 40% and 100% for non-treated subgroups [4].
In children, most THs result from a congenital defect in areas of the mesentery that is avascular and thin: transverse mesocolon, the sigmoid mesocolon and the ileocecal region. As a consequence, there are multiple theories of congenital causes of mesenteric tears [4]; due to the observed frequently in infants with atretic bowel segments, an etiologic relationship with prenatal intestinal ischemic accidents is likely [5]. However, in adults, THs are most often caused by previous gastrointestinal operations, intraperitoneal inflammation or trauma. In our case, the patient had no personal medical (intraperitoneal inflammation) or surgical history or trauma [6].
Clinically, internal hernias can be asymptomatic, or can cause chronic dyspepsia, vague epigastric pain, intermittent colicky periumbilical pain, nausea and vomiting [7, 8].
There is extreme difficulty in making diagnosis of internal hernia preoperatively and the most important diagnostic method is abdominal CT. Abdominal CT scan revealed a mildly dilated small bowel loops and a herniated sac through the transverse mesocolon. A herniation through an intraperitoneal orifice was identified. Awareness of these findings allows the radiologist to make the correct diagnosis of TH. The most helpful CT signs are: clustering of small bowel loops associated an abnormality in the mesenteric vessels, lack of omental fat between the loops and the anterior abdominal wall (sensitivity of 92%), a peripherally located small bowel (sensitivity of 85%) [9]. The herniated bowel lies outside the colon which is displaced centrally. In our case, abdominal CT revealed typical findings of TH.
An early diagnosis and treatment are required. It is important for surgeons to be familiar with the various types of internal hernias. The management of TH with acute intestinal obstruction requires: a nasogastric decompression, an initial resuscitation and a surgical procedure [10]. The surgical management includes reduction of herniated structures, resection of intestinal segments (in the presence of necrosis or perforation) and closure of hernial orifice (for prevention of recurrence of hernia). In our case, the symptoms were managed with conservative measures. We believe that conservative measures of TH is recommended in selected cases as it decreases the morbidity, mortality and significantly shortens the hospital stay. Our patient did not undergo operation so the imaging findings were not independently confirmed
Even in cases with no previous laparotomy, it is important to consider the possibility of TH in patients with signs and symptoms of intestinal obstruction, particularly in absence of external hernia or inflammatory intestinal disease. Prompt abdominal imaging is essential in making the correct diagnosis. Surgeons should be aware of the existence of this kind of atypical presentation of hernia.
Conflict of Interests Statement
There are no conflicts of interests.
| References | ▴Top |
- Martin LC, Merkle EM, Thompson WM. Review of internal hernias: radiographic and clinical findings. AJR Am J Roentgenol. 2006;186(3):703-717.
doi pubmed - Newsom BD, Kukora JS. Congenital and acquired internal hernias: unusual causes of small bowel obstruction. Am J Surg. 1986;152(3):279-285.
doi - Gomes R, Rodrigues J. Spontaneous adult transmesentric hernia with bowel gangrene. Hernia. 2011;15(3):343-345.
doi pubmed - Blachar A, Federle MP. Internal hernia: an increasingly common cause of small bowel obstruction. Semin Ultrasound CT MR. 2002;23(2):174-183.
doi - Murphy DA. Internal Hernias in Infancy and Childhood. Surgery. 1964;55 :311-316.
pubmed - Ueda J, Yoshida H, Makino H, Yokoyama T, Maruyama H, Hirakata A, Ueda H, et al. Transmesocolic hernia of the ascending colon with intestinal obstruction. Case Rep Gastroenterol. 2012;6(2):344-349.
doi pubmed - Yang DH, Chang WC, Kuo WH, Hsu WH, Teng CY, Fan YG. Spontaneous internal herniation through the greater omentum. Abdom Imaging. 2009;34(6):731-733.
doi pubmed - Hussein M, Khreiss M, Al-Helou G, Alaeddine M, Elias E, Abi Saad GS. Laparoscopic repair of a left paraduodenal hernia presenting with acute bowel obstruction: report of a case. Surg Laparosc Endosc Percutan Tech. 2012;22(1):e28-30.
doi pubmed - Takeyama N, Gokan T, Ohgiya Y, Satoh S, Hashizume T, Hataya K, Kushiro H, et al. CT of internal hernias. Radiographics. 2005;25(4):997-1015.
doi pubmed - Jung P, Kim MD, Ryu TH, Choi SH, Kim HS, Lee KH, Park JH. Transmesocolic hernia with strangulation in a patient without surgical history: case report. World J Gastroenterol. 2013;19(12):1997-1999.
doi pubmed
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Current Surgery is published by Elmer Press Inc.