

| Journal of Current Surgery, ISSN 1927-1298 print, 1927-1301 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Curr Surg and Elmer Press Inc |
| Journal website http://www.currentsurgery.org |
Original Article
Volume 7, Number 4, December 2017, pages 49-52
Patient Satisfaction Following Laparoscopic Umbilical Hernia Repair Using a “Two-Port” Technique
Ghassan Almaimani
Department of Surgery, Umm Al-Qura University, Alhijra Street, 21955 Makkah, Saudi Arabia
Manuscript submitted October 26, 2017, accepted December 15, 2017
Short title: Patient Satisfaction After Hernia Repair
doi: https://doi.org/10.14740/jcs333w
This article has been retracted
| Abstract | ▴Top |
Background: Measuring patient satisfaction is important to help improve health service delivery and improve outcomes. The aim of this study is to evaluate patient satisfaction with laparoscopic umbilical hernia repair and determine overall satisfaction with referral, outpatient consultation, pre-assessment clinic attendance, and post-operative care.
Methods: This was a retrospective study of 52 patients undergoing laparoscopic umbilical hernia repair. Each patient completed an extensive self-administered questionnaire distributed at a scheduled follow-up appointment 3 months following the operation.
Results: The response rate was 86.5%. Most patients (77.8%) were referred from their general practitioner. Patient satisfaction with surgical outcome was very high at > 98%, and the overall patient satisfaction from being listed for surgery to discharge was > 95%. Patient satisfaction was significantly associated with the patient being referred to the hospital by a general practitioner (GP).
Conclusions: Patient satisfaction is an important health outcome, and understanding the domains of satisfaction, as well as their relative importance to patients, is necessary to improve overall quality of patient care. Laparoscopic umbilical hernia repair using a “two-port” technique is an effective procedure with excellent results and an extremely high rate of patient satisfaction.
Keywords: Patient satisfaction; Umbilical hernia; Ventral hernia; Laparoscopy
| Introduction | ▴Top |
Patient satisfaction is a subjective concept that is difficult to measure. Many factors are known to influence patient satisfaction, but it is unknown which areas of care actually influence overall satisfaction. Traditionally, clinical success has been measured by the absence of complications. More recently, clinical outcomes have been assessed by patient-reported outcome measures (PROMs), where patient satisfaction is perhaps the most important criterion of success [1]. This concept is well recognized in the service industries but remains a nebulous concept in clinical care. The two-port laparoscopic hernia repair technique is reported to have the advantages of being the least minimally-invasive umbilical repair procedure described to date [2, 3]. Here we build on our recent study of surgical outcomes using the two-port laparoscopic hernia repair technique [4]. Although there have been several studies of patient outcomes after traditional hernia repair and laparoscopic repair using three- or four-port techniques, patient satisfaction after two-port umbilical hernia repair is unknown.
| Methods | ▴Top |
This was a retrospective study of 52 patients undergoing laparoscopic umbilical hernia repair at our hospital. Each patient completed an extensive self-administered questionnaire distributed at a scheduled follow-up appointment 3 months following the operation. Patients were surveyed on: 1) their referral route, 2) satisfaction with the surgical outpatient clinic service including any written information provided, 3) explanations provided before the preoperative assessment, and 4) satisfaction with surgical outcome. The care given to the patient before and after surgery was also assessed. All patients underwent hernia repair via the two-port technique. The Chi-squared test was used to examine associations between variables and patient satisfaction. Data were analysed in Excel v17.7 (Microsoft Corp., Redmond, WA).
| Results | ▴Top |
Forty-five of 52 patients responded (86.5%), with non-responding patients living abroad. Overall, 40% were male and 60% were female (Table 1). The majority (75%) of patients were 30 - 65 years old. Most patients (77.8%) were referred by their general practitioner. Thirty (66.7%) patients received their operation within 2 weeks of the surgical outpatient appointment.
 Click to view | Table 1. Patient Satisfaction Before, During, and After Laparoscopic Umbilical Hernia Repair |
Patient satisfaction with staff is shown in Figure 1. Overall, 43/45 (95.6%) patients were satisfied with their care. Positive comments included praising the service and the friendly, sympathetic, and professional care given by doctors, nurses, and clerks. Forty-three (43/45, 95.6%) patients were satisfied with the aesthetic outcome and barely visible scars. Negative comments related to the waiting time in the outpatient clinic, which was up to 2 h for some patients.
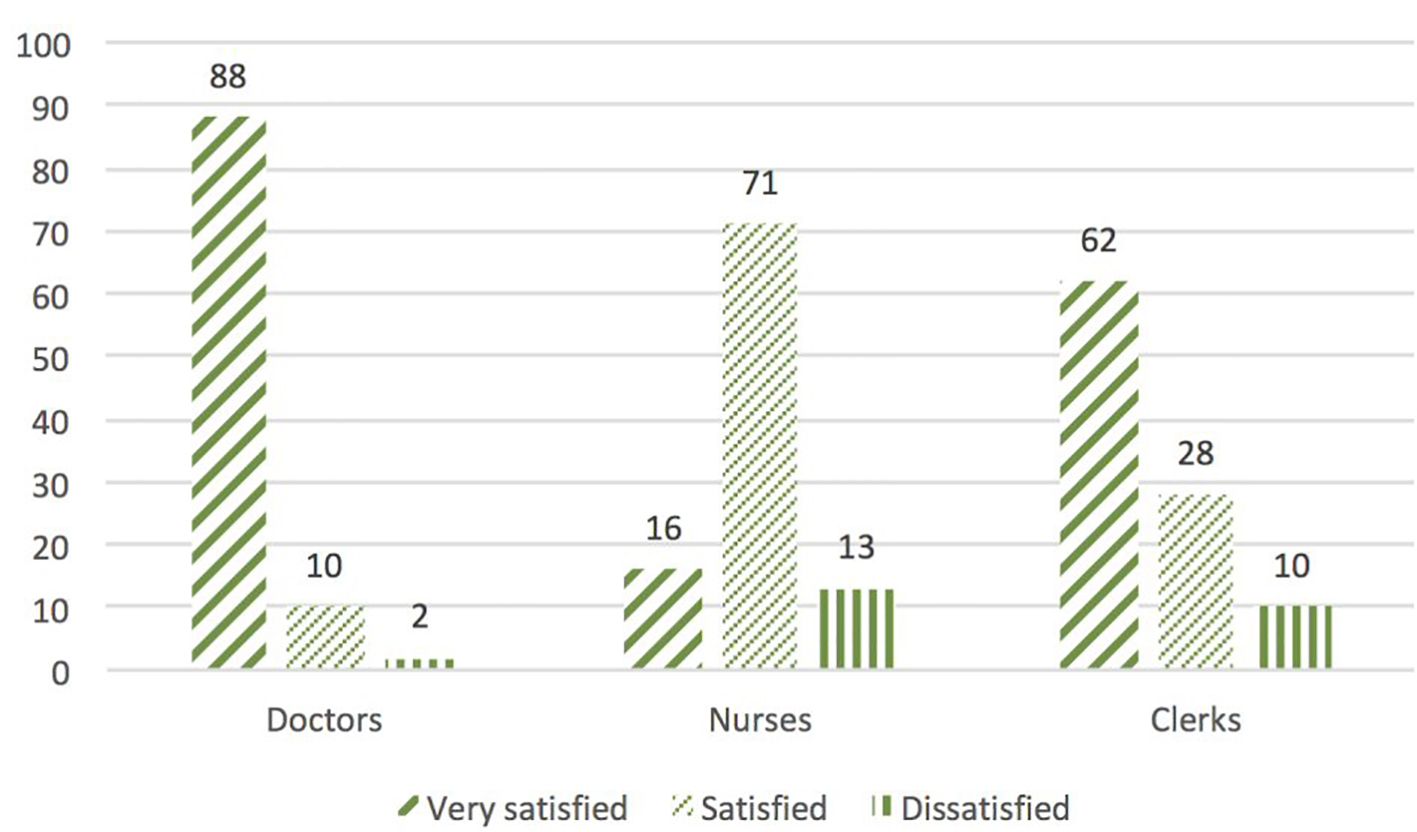 Click for large image | Figure 1. Patient satisfaction with staff. |
The Chi-squared test was used to examine associations between age, gender, and general practitioner (GP) referral and patient satisfaction after surgery. There was no association between age or gender and patient satisfaction but patient satisfaction was significantly associated with the patient being referred to the hospital by a GP.
| Discussion | ▴Top |
The ultimate goal of umbilical hernia repair is to improve and restore the patient’s quality of life. This is achievable, especially when due emphasis is given to patient-reported outcomes. Patient-reported outcomes have become one of the most important measures for assessing medical and surgical treatments [5, 6].
Satisfaction represents a subjective assessment rather than an objective measurement [7]. Multiple factors can influence the assessment of satisfaction such as preoperative expectations, the way in which patients are handled by staff, the information provided to patients [8], and surgical outcome [9]. The timing of administration of satisfaction surveys may also influence how patients report satisfaction; many surveys are conducted soon after surgery or before hospital discharge, which may produce different findings from surveys conducted several days or weeks later [7]. For example, Lemos et al [9] surveyed patient satisfaction after ambulatory surgery at discharge and 30 days after surgery. Complete satisfaction was reported in 75% of patients at discharge, which decreased to 62% at 30 days. The authors postulated that patient satisfaction was strongly influenced by clinical outcome at the later time point.
Chronic pain and recurrence after laparoscopic umbilical hernia repair adversely affect satisfaction. In our study, patient satisfaction with surgical outcome was very high at > 98%. Absence of chronic pain and recurrence and aesthetic outcome were the most important factors related to patient satisfaction after surgery in our study. Langbach et al [10] found that 60.5% of patients were satisfied even 10 years after laparoscopic ventral hernia repair, although a recurrence rate of 66.2% in that study could explain the relatively low satisfaction rates after longer periods of follow-up. Eriksen et al [11] reported that pain was associated with dissatisfaction after laparoscopic ventral hernia repair in the absence of recurrences, while Liang et al [12] reported 74.6% satisfaction following laparoscopic ventral hernia repair, with decreased patient satisfaction mainly associated with perception of poor cosmetic outcome and chronic pain.
As here, Wallin et al [13] reported that age and gender do not influence patient satisfaction after surgery. We found that the patient satisfaction was significantly increased when patients were referred to hospital by a GP. Guo et al [14] reported that patients need overall support from their doctor in order to be satisfied with treatment outcomes.
Comprehensive preoperative information causes little or no increase in overall patient anxiety [15]. Poor patient recall of verbal preoperative information is well documented [16, 17], and most respondents want written preoperative information. A standardized written information sheet may also be the best medium in which to mention rare complications, leaving time for the surgeon to verbally discuss patient-specific risks and postoperative expectations. In our study, patient satisfaction was significantly increased by giving them printed information.
This paper has some limitations. First, the survey was conducted 3 months after the operation, which may be too soon to assess optimal surgical outcomes or complications in terms of clinical recurrence. Second, the study population was relatively small. Finally, the satisfaction survey was a single question with “yes/no” responses, and this approach has been criticized as too simplistic to fully evaluate satisfaction [18].
Conclusions
Patient satisfaction is an important health outcome, and understanding the domains of satisfaction and their relative importance to patients is necessary to improve the overall quality of patient care. Laparoscopic umbilical hernia repair using a “two-port” technique is an effective procedure with excellent results and an extremely high rate of patient satisfaction.
Acknowledgments
We would like to thank all patients who participated in this study.
Conflict of Interest
The author declares no competing interests.
Financial Support
None.
| References | ▴Top |
- Hamilton DF, Lane JV, Gaston P, et al. What determines patient satisfaction with surgery? A prospective cohort study of 4709 patients following total joint replacement. BMJ Open. 2013;3:e002525.
doi pubmed - Abir F, Eisenberg D, Bell R. Laparoscopic ventral hernia repair using a two (5-mm) port technique. JSLS. 2005;9(1):94-96.
pubmed - Mehrotra PK, Ramachandran CS, Arora V. Two port laparoscopic ventral hernia mesh repair: an innovative technical advancement. Int J Surg. 2011;9(1):79-82.
doi pubmed - Almaimani G, Oyais A. Laparoscopic umbilical hernia repair using a "two-port" technique: a single-center experience. J Curr Surg. 2017;7:39-41.
doi - Turnbull JE, Luther KM. Patient satisfaction report paves way to improved care. QRC Advis. 1996;13(1):1-7.
pubmed - Wright JG. Evaluating the outcome of treatment. Shouldn’t We be asking patients if they are better? J Clin Epidemiol. 2000;53(6):549-553.
doi - Royse CF, Chung F, Newman S, Stygall J, Wilkinson DJ. Predictors of patient satisfaction with anaesthesia and surgery care: a cohort study using the Postoperative Quality of Recovery Scale. Eur J Anaesthesiol. 2013;30(3):106-110.
doi pubmed - Caljouw MA, van Beuzekom M, Boer F. Patient’s satisfaction with perioperative care: development, validation, and application of a questionnaire. Br J Anaesth. 2008;100(5):637-644.
doi pubmed - Lemos P, Pinto A, Morais G, Pereira J, Loureiro R, Teixeira S, Nunes CS. Patient satisfaction following day surgery. J Clin Anesth. 2009;21(3):200-205.
doi pubmed - Langbach O, Bukholm I, Benth JS, Rokke O. Long term recurrence, pain and patient satisfaction after ventral hernia mesh repair. World J Gastrointest Surg. 2015;7(12):384-393.
doi pubmed - Eriksen JR, Poornoroozy P, Jorgensen LN, Jacobsen B, Friis-Andersen HU, Rosenberg J. Pain, quality of life and recovery after laparoscopic ventral hernia repair. Hernia. 2009;13(1):13-21.
doi pubmed - Liang MK, Clapp M, Li LT, Berger RL, Hicks SC, Awad S. Patient Satisfaction, chronic pain, and functional status following laparoscopic ventral hernia repair. World J Surg. 2013;37(3):530-537.
doi pubmed - Wallin E, Lundgren P, Ulander K, Holstein C. Does age, gender or educational background affect patients’ satisfaction with short stay surgery? Ambulatory Surg. 2000;8:79-88.
doi - Guo Y, Kuroki T, Yamashiro S, Koizumi S. Illness behaviour and patient satisfaction as correlates of self-referral in Japan. Fam Pract. 2002;19(4):326-332.
doi pubmed - Newton-Howes PA, Bedford ND, Dobbs BR, Frizelle FA. Informed consent: what do patients want to know? N Z Med J. 1998;111(1073):340-342.
pubmed - Dawes P, Davison P. Informed consent: what do patients want to know? J Royal Soc Med. 1994;87:149-152.
pubmed - Nisselle P. Informed consent. N Z Med J. 1993;106(961):331-332.
pubmed - Chanthong P, Abrishami A, Wong J, Herrera F, Chung F. Systematic review of questionnaires measuring patient satisfaction in ambulatory anesthesia. Anesthesiology. 2009;110(5):1061-1067.
doi pubmed
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Current Surgery is published by Elmer Press Inc.