

| Journal of Current Surgery, ISSN 1927-1298 print, 1927-1301 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Curr Surg and Elmer Press Inc |
| Journal website http://www.currentsurgery.org/ |
Case Report
Volume 5, Number 1, April 2015, pages 143-145
Non-Communicating Bronchial Cyst Presenting as Cystic Thyroid Nodule
Tugba Han Yilmaza, Varlik Erola, d, Sevinc Eraslanb, Hasan Yerlic, Huseyin Gulaya
aDepartment of General Surgery, Practice and Research Center, Baskent University Zubeyde Hanim, Turkey
bDepartment of Internal Medicine, Dokuz Eylul University Faculty of Medicine, Turkey
cDepartment of Radiology, Practice and Research Center, Baskent University Zubeyde Hanim, Turkey
dCorresponding Author: Varlik Erol, Department of General Surgery, Practice and Research Center, Baskent University Zubeyde Hanim, Karsiyaka, Izmir, Turkey
Manuscript accepted for publication April 15, 2015
Short title: Non-Communicating Bronchial Cyst
doi: http://dx.doi.org/10.14740/jcs264w
| Abstract | ▴Top |
Bronchial cysts are congenital sacs that result from developmental anomaly of the primitive foregut. They are mainly encountered in the mediastinum, and cervical presentation is a rarity. We describe a case of a bronchial cyst that presented as a left lateral cervical mass mimicking cystic thyroid nodule in an adult. A literature review of this rare pathology is undertaken.
Keywords: Adult; Bronchogenic cyst; Cervical
| Introduction | ▴Top |
Cervical bronchogenic cysts are rare entity and result from the congenital malformation of the ventral foregut development and are usually diagnosed in the pediatric population. They usually present on the right side of the neck and they are extremely rare in adults [1]. Its prophylactic excision leads to excellent outcome [2-4]. We present a case of a bronchial cyst that presented as a left lateral cervical mass mimicking cystic thyroid nodule in an adult.
| Case Report | ▴Top |
A 41-year-old woman presented with a painless, smooth, hard in consistency 5 cm mass in the left anterior triangle of the neck. This was moving on swallowing and a provincial diagnosis of left thyroid mass was made. The rest of the history and clinical examination were insignificant. The thyroid function tests were within normal limits and the anti-TPO antibody (ANTI-M) was slightly raised. Thyroid ultrasonography showed a cystic lesion with heterogenic echogenicity involving the distal part of the left lobe of the thyroid. Isotope scan showed a cold nodule in the same area (Fig. 1) and it was followed by computed tomography imaging that confirmed the presence of a 5 × 6 cm smooth cystic lesion at the level of the lower part of left thyroid lobe. This was extending to the upper mediastinum causing deviation of the trachea to the right (Fig. 2).
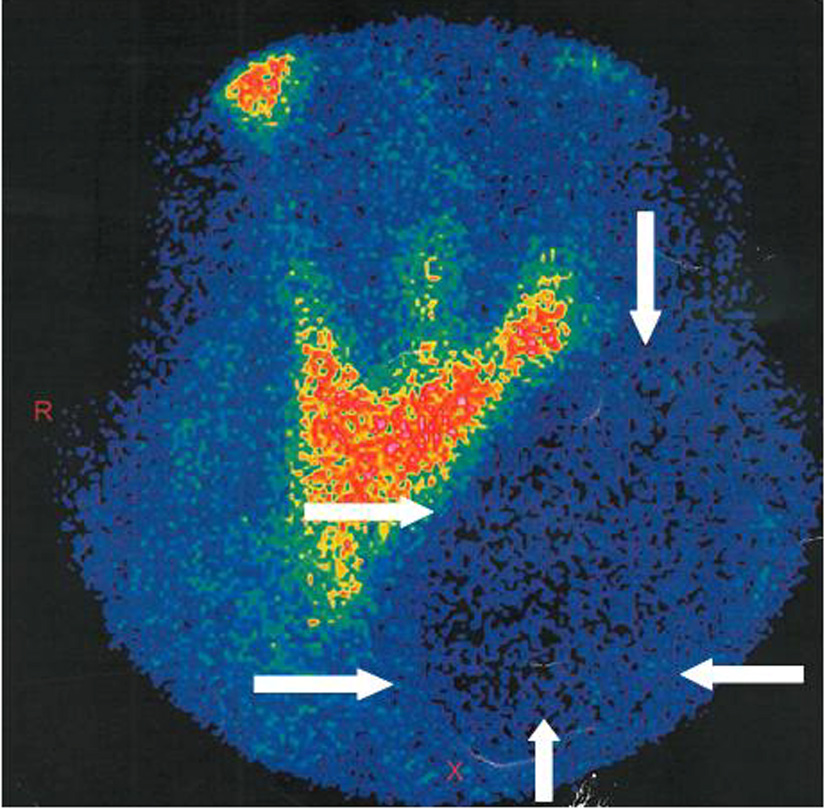 Click for large image | Figure 1. Thyroid scintigraphy of the patient. |
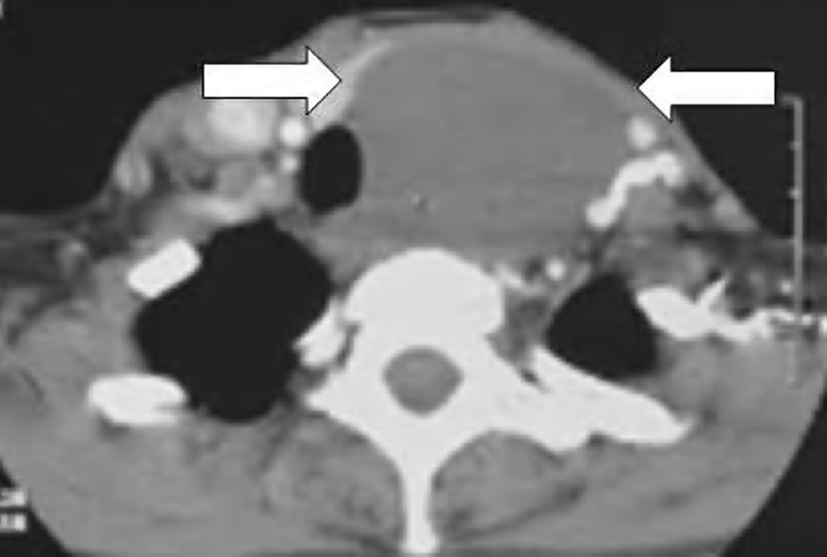 Click for large image | Figure 2. Computed tomography (CT) of the patient, showing the cystic lesion extending at the upper mediastinum. |
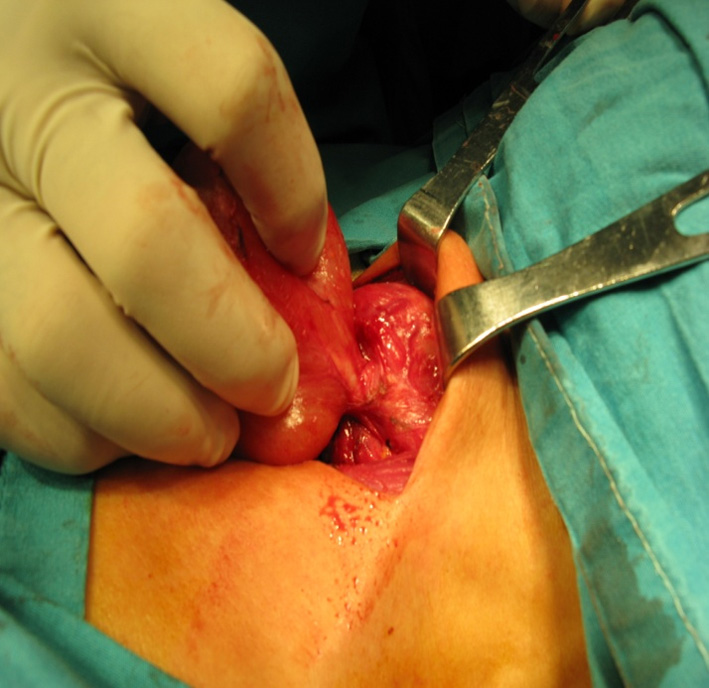
The patient was taken to the operating theater with a preoperative diagnosis of nodular goiter. At operation, through a collar incision, smooth-walled cystic lesion measuring 6 × 7 cm was found that was in contact but not in continuity to the lower pole of the left thyroid lobe (Fig. 3). This cyst was connected to the area between the second and third tracheal ring on the left, with a 3 mm long “cartilaginous band”. The cyst was dissected easily from the surrounding tissues (the extension to the anterior mediastinum was easily delivered into the operative field) and its connection to the trachea was transected. Although no lumen was observed, the “band” was ligated (Fig. 4). The cyst was opened at the end of the operation and it was found to contain clear mucinous fluid. The patient had good postoperative recovery and was discharged home next day. The histology report came back as cervical bronchogenic cyst with simple, columnar, ciliated respiratory epithelium and mucoid cells. There was a focus of chondroid tissue corresponding to the ligated “cartilaginous band” (Fig. 5). The patient was followed up for 2 years with no evidence of recurrence of the cyst.
 Click for large image | Figure 3. A smooth-walled cystic lesion measuring approximately 6 × 7 cm. |
 Click for large image | Figure 4. Tracheal attachment area including discoid cartilage tissue. |
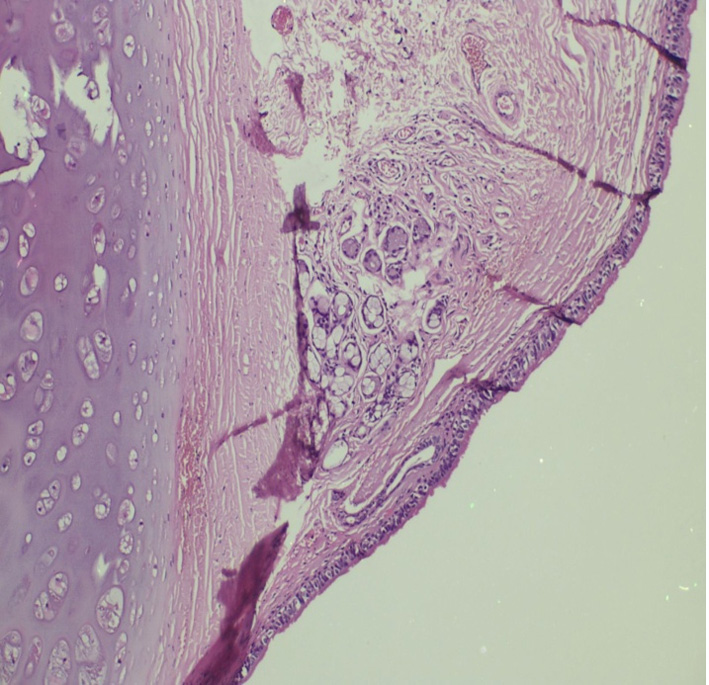 Click for large image | Figure 5. Respiratory columnar, ciliated epithelium lining the cervical bronchial cyst and mucoid cells with a focus of chondroid tissue. |
| Discussion | ▴Top |
Bronchogenic cysts are rare congenital malformations of ventral foregut development and are usually located in the mediastinum or intrapulmonary regions. Location in the cervical area is uncommon and the majority of cases reported affected the pediatric population. There are only a few reports of cervical bronchogenic cysts presenting in adults [5, 6]. As bronchogenic cysts develop from evaginations of embryologic tracheal buds, they may well develop anywhere along the trachea. Due to the fact that the esophagus deviates to the left of the cervical trachea, most of the cysts present on the right side of the neck. In our case, the cyst was left sided, a rare occurrence.
Bronchogenic cyst apart from causing cosmetic problems to the patient may produce pressure symptoms to the surrounding structures expressing themselves as stridor, dyspnea or dysphagia. Infection of the bronchogenic cyst is another complication, as is in rare cases the development of malignancy.
Differential diagnosis includes thyroidal cysts, metastatic lymph nodes [7], abscesses, hydatic cysts, other tracheal malformations and infected tracheal diverticula. This should also include other congenital malformations such as tracheitis, tracheal bronchus, tracheal cleft, and congenitally short tracheas. As bronchogenic cysts presenting in the cervical area will move with swallowing due to their attachment to the trachea, differential diagnosis from thyroid masses can be very difficult, if it happens to be located near the thyroid. Advanced imaging methods such as computed tomography or magnetic resonance imaging and also bronchoscopy might be needed. Particularly magnetic resonance imaging may show the presence of an attachment/continuity between the trachea and the cyst. Even after all these investigations, the surgeon can take the patient to theater without a solid preoperative diagnosis. The intraoperative finding of an attachment to the trachea will suggest the diagnosis and the histological report will give confirmation. In most reported cases, the attachment of the cyst to the trachea contained a lumen. This was not true in our case as there was complete lack of lumen, a fact observed intraoperatively and also confirmed histologically.
The treatment of bronchogenic cysts in children is dissection. On the other hand, in adults different options may be considered [8]. Simple survey has been recommended as a viable proposition in small and asymptomatic extrapulmonary cysts [9]. Resection is considered mandatory with intrapulmonary cysts as the high frequency of bronchocystic fistula renders a high spontaneous complication rate [9]. A minimally invasive option has been described with transbronchial or mediastinoscopic needle decompression [10]. However, most authors recommend routine surgical excision. Needless to say that in case of malignant change, resection of the cyst by open procedure is probably a more oncologically acceptable operation [2, 3]. The rare intraoperative complication of fatal air embolism has not been described in open surgery [4]. Yoshida et al reported a case with tracheal wall damage while performing sharp separation of the cystic wall from the trachea with thoracoscopic surgery [11].
In conclusion, bronchogenic cysts of the cervical area are a rare occurrence that should be considered in the differential diagnosis of cystic masses moving with swallowing. Although magnetic resonance imaging has gotten a significant advantage of establishing a preoperative diagnosis, in most cases the patient will be taken to theater without a solid preoperative diagnosis. The cyst should be approached through a cervical incision even if it is “plunging” in the anterior mediastinum. The operative finding of a connection to the trachea will suggest the diagnosis, but these must be confirmed by histology. Open resection of cervical bronchogenic cyst is at present the recommended method of management.
Conflict of Interests
The authors declare that there is no conflict of interests regarding the publication of this paper.
| References | ▴Top |
- Newkirk KA, Tassler AB, Krowiak EJ, Deeb ZE. Bronchogenic cysts of the neck in adults. Ann Otol Rhinol Laryngol. 2004;113(9):691-695.
doi pubmed - St-Georges R, Deslauriers J, Duranceau A, Vaillancourt R, Deschamps C, Beauchamp G, Page A, et al. Clinical spectrum of bronchogenic cysts of the mediastinum and lung in the adult. Ann Thorac Surg. 1991;52(1):6-13.
doi - Ribet ME, Copin MC, Gosselin B. Bronchogenic cysts of the mediastinum. J Thorac Cardiovasc Surg. 1995;109(5):1003-1010.
doi - Bocciolini C, Dall'olio D, Cunsolo E, Latini G, Gradoni P, Laudadio P. Cervical bronchogenic cyst: asymptomatic neck mass in an adult male. Acta Otolaryngol. 2006;126(5):553-556.
doi pubmed - Dubois P, Belanger R, Wellington JL. Bronchogenic cyst presenting as a supraclavicular mass. Can J Surg. 1981;24(5):530-531.
pubmed - Hadjihannas E, Ray J, Rhys-Williams S. A cervical bronchogenic cyst in an adult. Eur Arch Otorhinolaryngol. 2003;260(4):216-218.
pubmed - Jun HH, Kim SM, Lee YS, Hong SW, Chang HS, Park CS. Cervical bronchogenic cysts mimic metastatic lymph nodes during thyroid cancer surgery. Ann Surg Treat Res. 2014;86(5):227-231.
doi pubmed - Barsotti P, Chatzimichalis A, Massard G, Wihlm JM. Cervical bronchogenic cyst mimicking thyroid adenoma. Eur J Cardiothorac Surg. 1998;13(5):612-614.
doi - Ginsberg RJ, Atkins RW, Paulson DL. A bronchogenic cyst successfully treated by mediastinoscopy. Ann Thorac Surg. 1972;13(3):266-268.
doi - Naunheim KS, Andrus CH. Thoracoscopic drainage and resection of giant mediastinal cyst. Ann Thorac Surg. 1993;55(1):156-158.
doi - Yoshida M, Kondo K, Toba H, Kenzaki K, Sakiyama S, Tangoku A. Two cases of bronchogenic cyst with severe adhesion to the trachea. J Med Invest. 2007;54(1-2):187-190.
doi pubmed
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Current Surgery is published by Elmer Press Inc.