

| Journal of Current Surgery, ISSN 1927-1298 print, 1927-1301 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Curr Surg and Elmer Press Inc |
| Journal website https://www.currentsurgery.org |
Case Report
Volume 12, Number 1, March 2022, pages 24-28

Innovative Utilization of Robotic-Assisted Laparoscopy for Repair of Perforated Anterior Duodenal and Posterior Gastric Ulcer at a Hospital With Twenty-Four-Hour da Vinci Xi Capabilities
Rachel Gantza, Robert Azarb, c, Greg Starleyb
aDepartment of Medical Education, College of Osteopathic Medicine of the Pacific NW, Western University of Health Sciences, Lebanon, OR 97355, USA
bGeneral Surgery, Legacy Mount Hood Medical Center, Gresham, OR 97030, USA
cCorresponding Author: Robert Azar, General Surgery, Legacy Mount Hood Medical Center, Gresham, OR 97030, USA
Manuscript submitted January 19, 2021, accepted February 18, 2021, published online March 29, 2022
Short title: Innovative Repair of Perforated Ulcers
doi: https://doi.org/10.14740/jcs435
| Abstract | ▴Top |
Robotic-assisted laparoscopic surgical methods have become increasingly more common in general surgery in the recent years. However, emergency utilization of this surgical method has not been studied in depth. Herein we present two cases of perforations located on the posterior gastric and anterior duodenal surfaces successfully repaired utilizing the robotic-assisted laparoscopic approach in a hospital that has 24-h da Vinci Xi capabilities.
Keywords: Emergency; da Vinci Xi; Posterior gastric perforation; Anterior duodenal perforation
| Introduction | ▴Top |
Robotic laparoscopic surgery compared to standard laparoscopic surgery removes the counter-intuitive motion, aligns the eyes and hands, has improved ergonomics, and has increased degrees of motion [1]. These improvements have allowed for robotic surgery to become highly utilized in elective surgery throughout surgical subspecialties. In the area of general surgery, these methods have become increasingly more common with an increase from 1.8% to 15.1% of procedures in the 2012 to 2018 timeframe [2]. However, the utilization of robotic-assisted laparoscopic surgical methods in general surgery emergent cases has not been extensively reported. The goal of this case report is to demonstrate the efficacy and successful utilization of the robotic-assisted laparoscopic approach in emergent presentations of perforated gastric and duodenal ulcer.
| Case Reports | ▴Top |
Case 1
Investigations
Patient number one was a 40-year-old healthy Chinese speaking male with no significant past medical or surgical history presented with periumbilical and epigastric abdominal pain for 1 week. He had been evaluated the previous day and discharged with a diagnosis of enteritis. The patient returned with abdominal pain that was diffuse, constant, dull, intermittently sharp, and rated 8/10. On physical exam he appeared in no acute distress, but had diffuse abdominal tenderness to palpation. His complete blood count (CBC) and lipase were within normal limits. A computed tomography (CT) scan with contrast showed suspected bowel perforation due to pneumoperitoneum and ascites, and the stomach displayed extensive hyperemia and wall thickening (Fig. 1a, b).
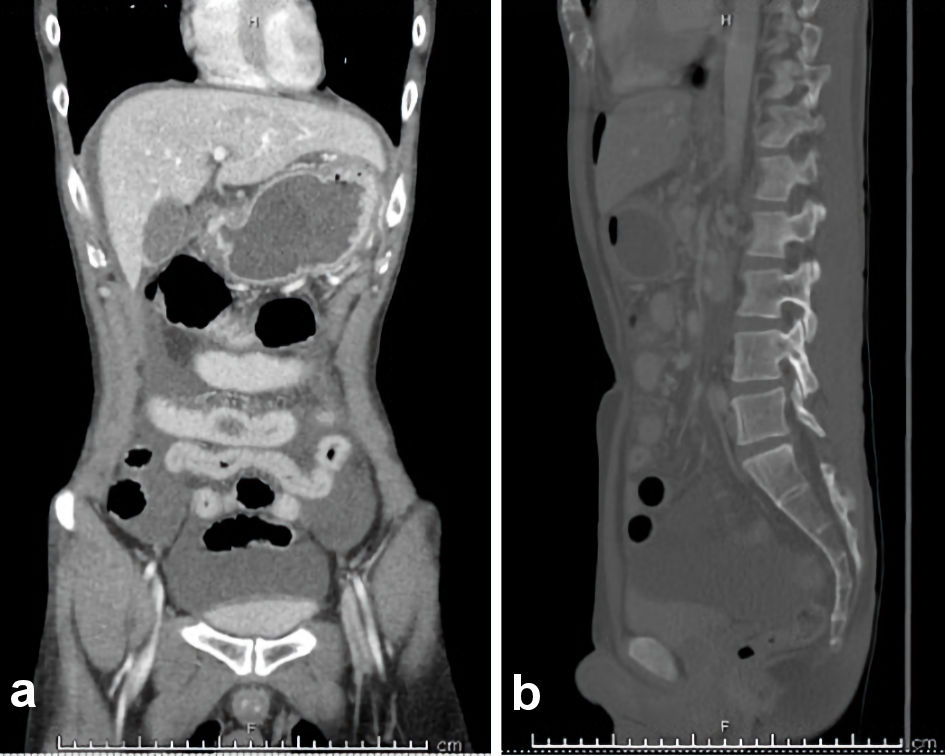 Click for large image | Figure 1. (a, b) CT with contrast revealing gastritis and pneumoperitoneum (case 1). CT: computed tomography. |
Diagnosis
Patient was suspected to have a bowel perforation of unknown location due to pneumoperitoneum and ascites displayed on CT with contrast. Patient was emergently taken to surgery, and laparoscopy revealed a 1.5-cm perforation on the anterior duodenal bulb (Fig. 2).
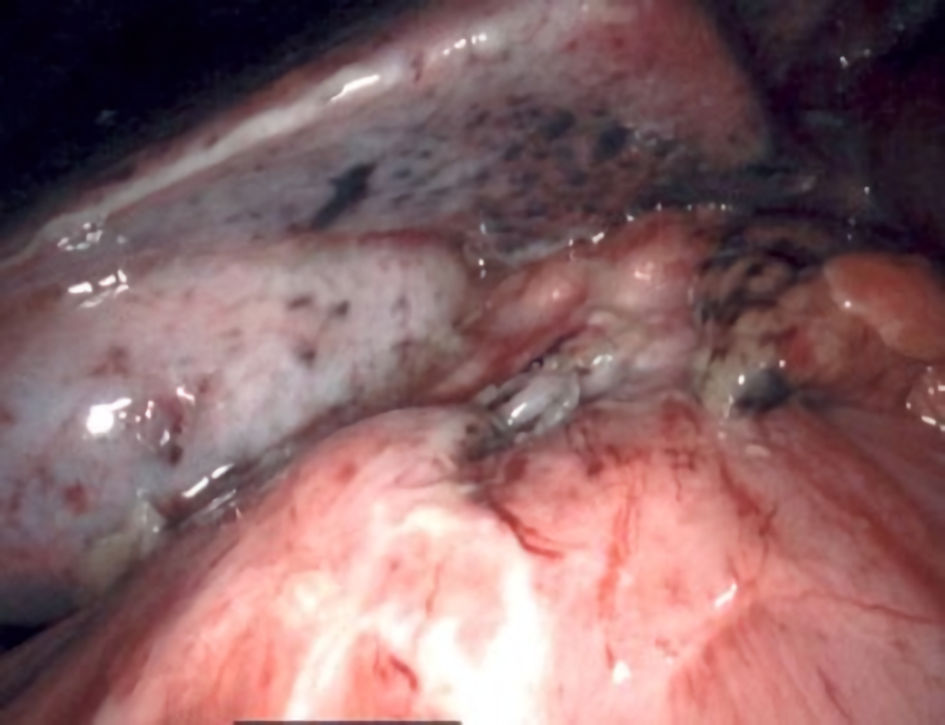 Click for large image | Figure 2. Visualization of anterior duodenal bulb ulcer measuring approximately 1.5 cm (case 1). |
Treatment
The laparoscopy was converted to a robotic-assisted approach using three ports. The 1.5-cm anterior perforated duodenal bulb ulcer was visualized (Fig. 2), repaired with 3-0 Vicryl (Fig. 3), and reinforced with an omental patch. There was no particulate contamination visualized, and irrigation was completed using warm saline solution. A 19 French JP drain and nasogastric (NG) tube were placed during surgery.
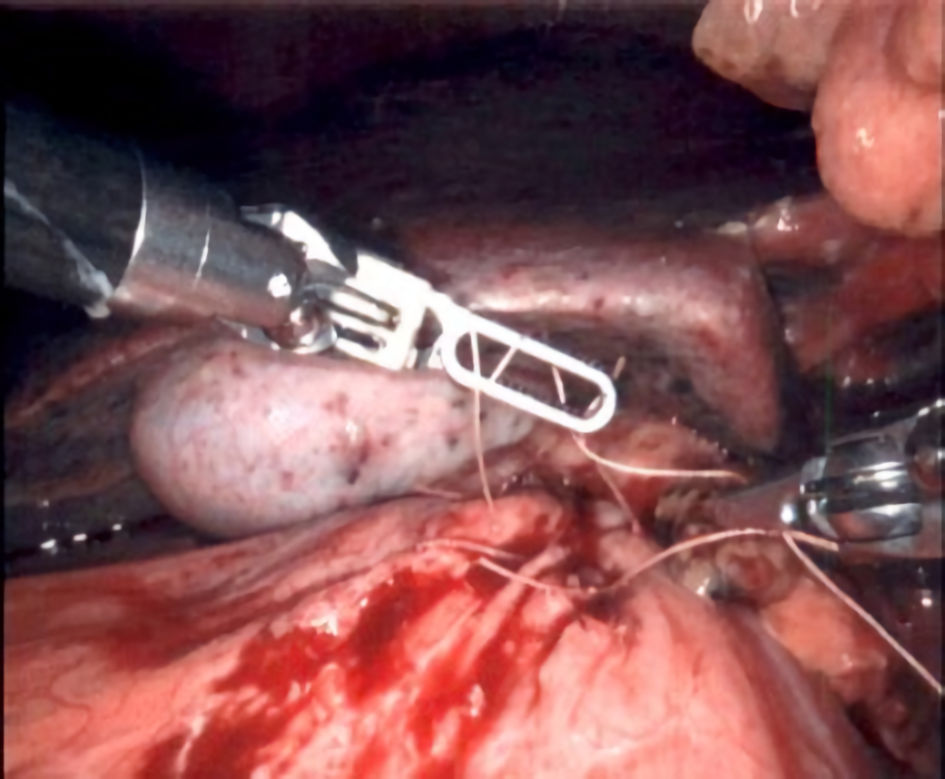 Click for large image | Figure 3. Repair of anterior duodenal bulb ulcer with 3-0 Vicryl (case 1). |
Follow-up and outcomes
On postoperative day 2, the small bowel follow-through showed no evidence of leak (Fig. 4). Patient was discharged on postoperative day 5 with minimal pain and tolerating a low residue diet. His pathology report returned positive for Helicobacter pylori (H. pylori). Patient returned to China and did not follow-up.
 Click for large image | Figure 4. Small bowel follow-through results on postoperative day 2 revealing no signs of contrast extravasation to suggest a leak (case 1). |
Case 2
Investigations
Patient number two was a 58-year-old female with a 60-pack year history of smoking, non-small cell lung cancer status post (s/p) lung resection, peripheral vascular disease and gastrointestinal (GI) bleed secondary to gastric ulcers, who was brought in by ambulance with gradually worsening abdominal pain over a 3-h period. The abdominal pain was diffuse and severe. On physical exam, patient had diffuse abdominal rebound tenderness. Labs showed an elevated white blood cell count. A CT scan revealed moderate pneumoperitoneum and free fluid suggestive of a perforated gastric ulcer (Fig. 5).
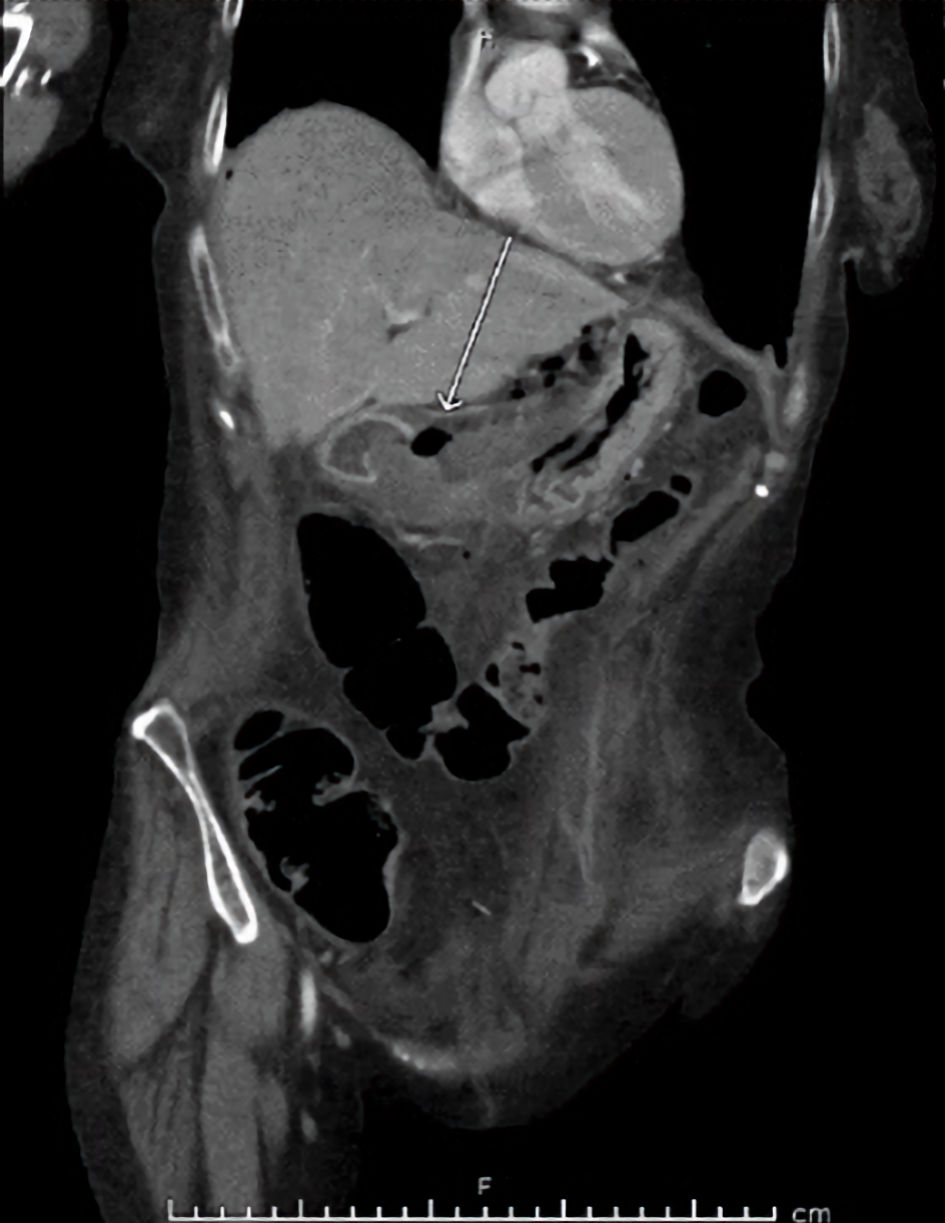 Click for large image | Figure 5. CT with contrast at initial presentation to emergency department revealing pneumoperitoneum and likely perforated gastric ulcer (arrow, case 2). CT: computed tomography. |
Diagnosis
Patient was suspected to have a gastric perforation along the antrum after CT scan with contrast displayed pneumoperitoneum and free fluid. Diagnostic laparoscopy followed by robotic assistance identified a 2-cm perforation located on the posterior aspect of the proximal pyloric channel (Fig. 6).
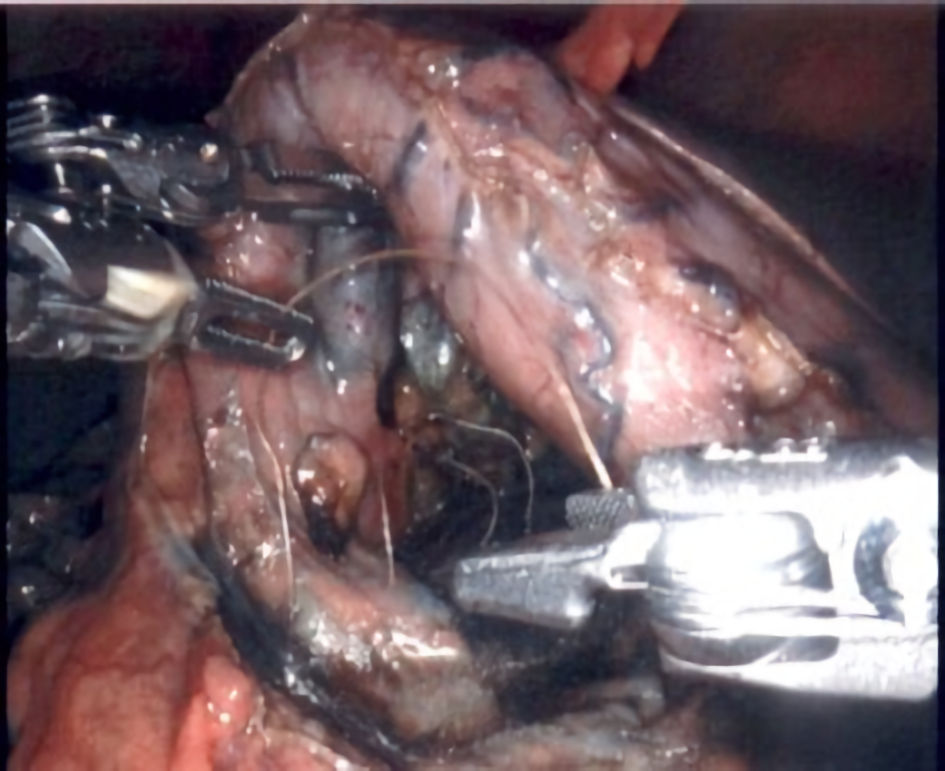
 Click for large image | Figure 6. Visualization of posterior pyloric channel ulcer measuring approximately 2 cm with utilization of methylene blue (case 2). |
Treatment
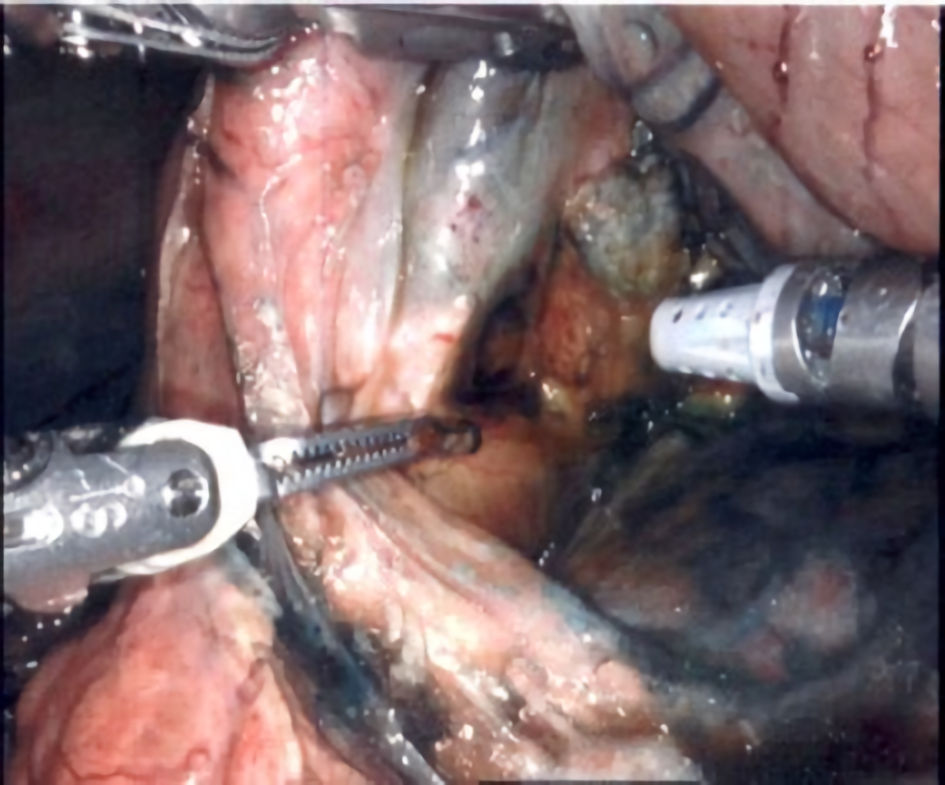
She was taken urgently to surgery, and laparoscopy revealed inflammation at the gastric antrum. The da Vinci Xi was then docked using four ports. A 2-cm perforation was located on the posterior aspect of the proximal pyloric channel with the utilization of methylene blue via patients’ NG tube (Fig. 6). There was diffuse bilious peritonitis with no solid particulate material. A biopsy of the ulcer and adjacent lesser omentum was collected. The perforation was closed utilizing interrupted 3-0 Vicryl suture (Fig. 7). An omental patch reinforcement was placed. Warm saline was used to irrigate the lesser sac. A 19 French JP drain and NG tube were placed.
 Click for large image | Figure 7. Posterior gastric perforation being repaired with 3-0 Vicryl (case 2). |
Follow-up and outcomes
On postoperative day 2, a small bowel follow-through showed no evidence of contrast extravasation (Fig. 8). Her hospital stay was prolonged by bilateral pleural effusions that improved with diuresis. She was discharged on postoperative day 14 on a low residue diet to a skilled nursing facility in stable condition. On follow-up, patient reported no pain, and physical exam revealed the laparoscopic incisions were healing appropriately. Pathology report was negative for malignancy and H. pylori. For next steps, patient will remain on Prilosec twice a day (BID) and will follow up with GI for esophagogastroduodenoscopy (EGD) in 1 month.
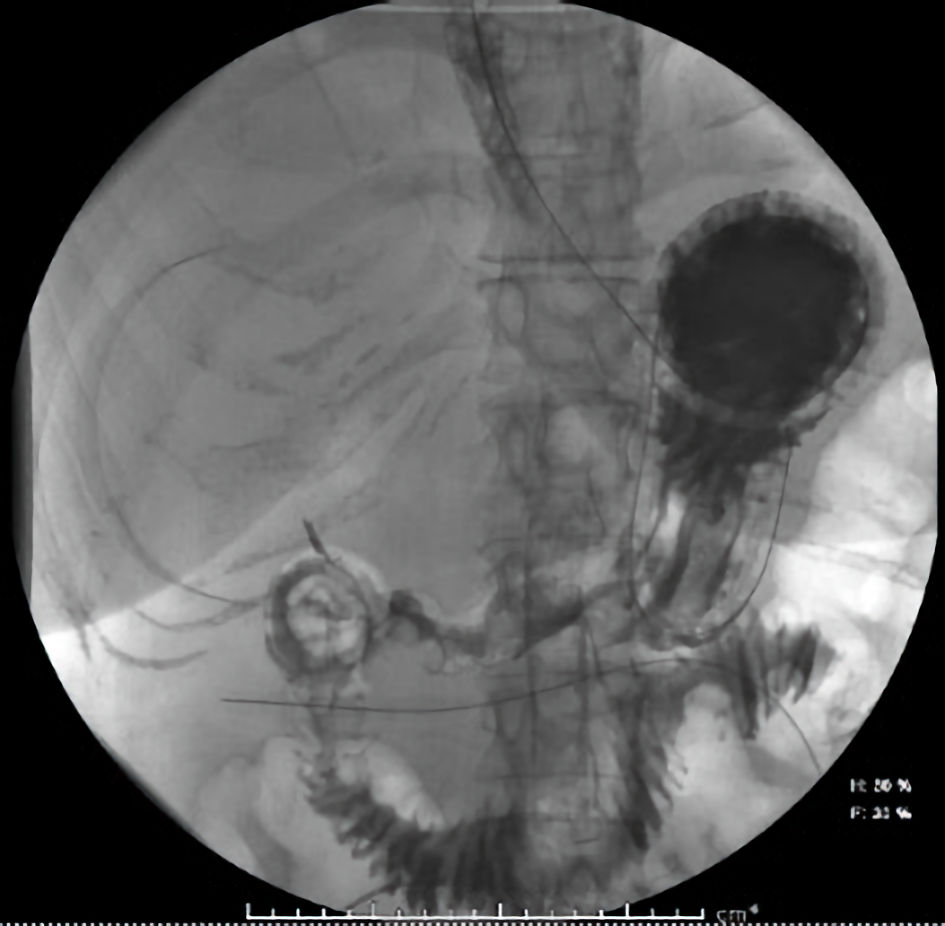 Click for large image | Figure 8. Small bowel follow-through results on postoperative day 2 revealing no signs of contrast extravasation to suggest a leak (case 2). |
| Discussion | ▴Top |
According to the World Society of Emergency Surgeons the reported annual incidence of perforation ranges from 0.004% to 0.014%, with sample size-weighted average 30-day mortality of 23.5%. The current guideline with level 2B evidence for emergent surgery in stable patients is to perform laparoscopic surgery over an open approach [3]. Laparoscopic procedural methods are specifically preferred due to having lower infection rates and decreased postoperative pain [4]. Additionally, one retrospective analysis showed laparoscopic surgery had a decreased length of stay and decreased pulmonary complications compared to the open approach [5]. Although robotic-assisted surgery continues to expand in the field of general surgery, little data exist regarding the benefits in emergent cases. In our review, one other case report was identified that demonstrated the successful robotic-assisted laparoscopic repair in a patient with delayed presentation of a perforated duodenal ulcer [6]. Thus, the hope with this case report is to add to the existing evidence of the utilization of the robotic-assisted laparoscopic approach in emergent small bowel and gastric perforations.
In the cases presented, both patients benefited from a robotic-assisted laparoscopic repair due to the improved operator ergonomics, increased degrees of motion and most importantly the improved visualization of the ulcers during the procedure. It is important to note that both patients had differing health profiles. Patient one was a healthy 40-year-old man with no significant past medical history while patient two was a 58-year-old woman with extensive smoking history, non-small cell lung cancer s/p lung resection, and peripheral vascular disease. This demonstrates that a robotic-assisted laparoscopic approach may be considered not only for patients that are in relatively good health but also patients that would most likely have a more challenging recovery if an open procedure was required.
Another important takeaway is the posterior location of the ulcer in patient two. In one review, the posterior location of perforated peptic ulcer was very rare (1.7% of gastric perforations) [7, 8]. Although many anterior ulcers can be easily visualized and repaired laparoscopically, those in other locations are more difficult. In this surgeon’s experience, the robotic capabilities allowed excellent visualization and repair of the posterior perforation located adjacent to the gastroduodenal artery. In this case, the robotic approach prevented laparotomy.
One hesitation for the use of robotics in emergent cases is management of patients who are unstable. Currently, studies have created algorithms for robotic emergency conversion and are becoming more and more standardized as the increase in robotic procedures are becoming more common [9]. Fortunately, the patients in this case report remained hemodynamically stable throughout the procedure, and there was no need for conversion to a laparoscopic or open approach.
The overall goal of this case report is to display how the da Vinci Xi can be successfully used in emergent perforated gastric and duodenal ulcers. The benefits of the robotic approach should be considered in these cases if available.
Learning points
The key takeaway from this case report is that the robotic-assisted laparoscopic approach can be successfully utilized in emergent cases of gastric and duodenal perforations. In these cases, specifically the posterior gastric perforation, the surgeon found that the robotic approach allowed for excellent visualization compared to a laparoscopic or open approach.
Acknowledgments
None to declare.
Financial Disclosure
None to declare.
Conflict of Interest
None to declare.
Informed Consent
Informed consent was obtained.
Author Contributions
Rachal Gantz contributed to the literature search and writing of manuscript. Robby Azar contributed to the design and performed surgeries. Greg Starley contributed to the design.
Data Availability
The data supporting the findings of this study are available on request from the corresponding author.
Declaration
The views that are expressed in this case report are the authors’ and are not an official position of Western University of the Health Sciences COMP-NW or Legacy Mount Hood Medical Center.
| References | ▴Top |
- Wilson EB. The evolution of robotic general surgery. Scand J Surg. 2009;98(2):125-129.
doi pubmed - Sheetz KH, Claflin J, Dimick JB. Trends in the adoption of robotic surgery for common surgical procedures. JAMA Netw Open. 2020;3(1):e1918911.
doi pubmed - Tarasconi A, Coccolini F, Biffl WL, Tomasoni M, Ansaloni L, Picetti E, Molfino S, et al. Perforated and bleeding peptic ulcer: WSES guidelines. World J Emerg Surg. 2020;15:3.
doi pubmed - Cirocchi R, Soreide K, Di Saverio S, Rossi E, Arezzo A, Zago M, Abraha I, et al. Meta-analysis of perioperative outcomes of acute laparoscopic versus open repair of perforated gastroduodenal ulcers. J Trauma Acute Care Surg. 2018;85(2):417-425.
doi pubmed - Gabriel V, Grigorian A, Schubl SD, Pejcinovska M, Won E, Lekawa M, Bernal N, et al. Perforated peptic ulcer surgery: decreased length of stay but no difference in mortality with laparoscopic repair. Surg Laparosc Endosc Percutan Tech. 2018;28(6):410-415.
doi pubmed - Omental patch repair for perforated duodenal ulcer: robotic approach in a patient with delayed presentation - SAGES Abstract Archives. SAGES. Accessed December 12, 2020. https://www.sages.org/meetings/annual-meeting/abstracts-archive/omental-patch-repair-for-perforated-duodenal-ulcerrobotic-approach-in-a-patient-with-delayed-presentation/.
- Badawy. A large posterior perforation of gastric ulcer: a rare surgical emergency. Accessed December 14, 2020. http://www.ejs.eg.net/article.asp?issn=1110-1121;year=2016;volume=35;issue=1;spage=74;epage=76;aulast=Badawy.
doi - Wong CH, Chow PK, Ong HS, Chan WH, Khin LW, Soo KC. Posterior perforation of peptic ulcers: presentation and outcome of an uncommon surgical emergency. Surgery. 2004;135(3):321-325.
doi pubmed - Ackah RL, Kenawy DM, Merritt RE, Kneuertz PJ. Preparing for the worst: universal algorithm for robotic surgery emergency conversion. J Am Coll Surg. 2021;232(2):220-222.
doi pubmed
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Current Surgery is published by Elmer Press Inc.