

| Journal of Current Surgery, ISSN 1927-1298 print, 1927-1301 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Curr Surg and Elmer Press Inc |
| Journal website https://www.currentsurgery.org |
Original Article
Volume 12, Number 2, December 2022, pages 38-44

Prevalence and Associated Factors of Post-Thrombotic Syndrome in Patients With Deep Vein Thrombosis
Shashi Praba Abeyrathnaa, Chandima Kulathilakea, b, Indira Wijesiriwardenaa
aDepartmet of Pathology, Faculty of Medical Sciences, University of Sri Jayewardenepura, Gangodawila, Nugegoda, Sri Lanka
bCorresponding Author: Chandima Kulathilake, Department of Pathology, Faculty of Medical Sciences, University of Sri Jayewardenepura, Gangodawila, Nugegoda 10250, Sri Lanka
Manuscript submitted April 17, 2022, accepted May 6, 2022, published online June 2, 2022
Short title: Prevalence and Associated Factors of PTS
doi: https://doi.org/10.14740/jcs459
| Abstract | ▴Top |
Background: Post-thrombotic syndrome (PTS) occurs as a long-term complication of deep vein thrombosis (DVT). The aim of this study was to evaluate the prevalence of PTS and its associated factors in a cohort of patients with lower extremity DVT in Sri Lanka.
Methods: A descriptive cross-sectional study was conducted in 80 patients who were assessed 6 months to 2 years after the acute episode of DVT. They were assessed using Vilalta scale to diagnose and grade the severity of PTS, anthropometry to calculate body mass index (BMI), duplex ultrasound scans, patients’ clinic record including international normalized ratio (INR) charts and an interviewer administered questionnaire. Categorical data were analyzed using Chi-square test and continuous variables were analyzed using analysis of variance (ANOVA) to determine association.
Results: Prevalence of PTS was 45.5% (36/80) according to Villalta scale. Recurrent DVT (P = 0.0002), high BMI (P = 0.073), and previous venous in competence (P = 0.032), showed significant association with PTS. Proximal DVT demonstrated a strong association with PTS (P = 0.002). Residual thrombosis at 3 months was strongly associated with PTS (P < 0.001), however, with a bias of very low sample with repeat duplex at 3 months post event. Awareness of PTS was extremely low (n = 0, 0%). Practice of elastic compression stockings (ECSs) use as a preventative measure of PTS failed to show any significant association (P = 0.61).
Conclusions: This study showed a significant prevalence of PTS among patients with previous DVT. Development of PTS is probably multi factorial. A validated risk assessment tool should be used to identify at-risk patients as prevention is the best approach to this irreversible morbidity.
Keywords: Post-thrombotic syndrome; Deep vein thrombosis; Elastic compression stockings
| Introduction | ▴Top |
Post-thrombotic syndrome (PTS) is a frequent long-term complication of deep vein thrombosis (DVT). It is defined as a collection of chronic venous symptoms and/or signs secondary to DVT [1].
The reported incidence of PTS varies widely. Various studies have reported different incidence rates for PTS ranging from 20% to 80% following acute DVT [2-4]. However, research done using validated diagnostic criteria estimates it to be as high as 50% despite adequate anticoagulation [4, 5]. Peak incidence of PTS is within the first 1 to 2 years [2], but the cumulative incidence of PTS continues to rise up at 20 years after the initial acute DVT [6]. No incidence or prevalence rates for Sri Lankan population exist to date.
Characteristic signs of PTS include limb edema, perimalleolar or extensive telangiectasia, venous ecstasia, hyper pigmentation, skin indurations and ulceration [7, 8]. In the long run they can develop tender pigmented thickening of the subcutaneous tissue called lipodermatosclerosis. The worst complication of PTS is venous ulceration, which is characteristically chronic, painful, slow to heal and even recurrent [9, 10]. PTS is the commonest cause of venous ulceration [6].
Diagnosis of PTS should only be attempted 3 - 6 months after an acute DVT, when symptoms due to DVT itself are no longer present. Even though there are invasive and noninvasive methods that support the diagnosis, in practice PTS is diagnosed mainly by using simple clinical scores.
There are several clinical scores, which include Widmer scale [11], Villalta scale [12], the Ginsberg measure [13], and CEPA system [14, 15]. Among these Villalta scale and CEPA system take the lead. However, agreement between these scores is poor; and they are not complementary to each other [16].
As an act in standardizing the diagnosis of PTS in clinical studies, subcommittee on control of anticoagulation of the International Society of Thrombosis and Hemostasis (ISTH) has recommended Villalta scale to be used in the diagnosis and grading of PTS [17]. Therefore, Villalta scale is used as the clinical tool in the diagnosis and grading severity of PTS in this study. Villalta scale (Fig. 1) [12] uses five symptoms and six signs as its determinants. Each component is graded (0 - 3) according to severity and the cumulative score is used to diagnose and grade PTS. It can also be used as a binary score to diagnose PTS. Also, it can be used to measure the response to treatment as well [18].
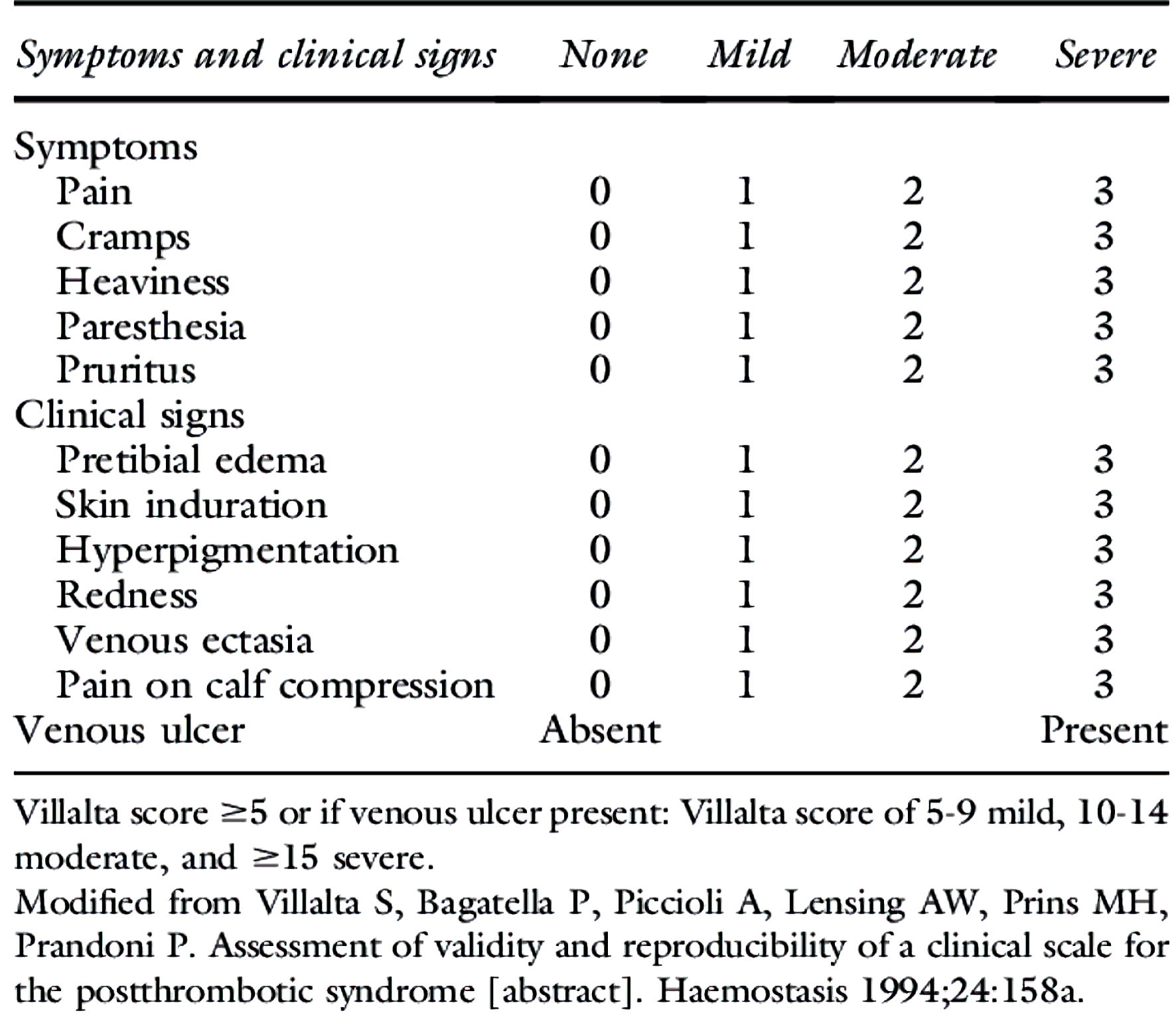 Click for large image | Figure 1. Villalta score. |
Though it has been recommended by ISTH in the diagnosis of PTS, awareness and application of the score in Sri Lankan clinical practice are very limited.
Several risk factors have been shown to be associated with the development of PTS. Various studies have highlighted several factors including sub therapeutic international normalized ratio (INR) [19], proximal thrombosis, higher body mass index (BMI), older age, female sex and previous ipsilateral venous thrombosis [20] as associated risk factors. Residual thrombosis and superficial valvular reflux were also highlighted in one study [21]. Persistently elevated D-dimer levels after initial 3 - 4 months has also been identified as a risk factor in several studies [22, 23].
In the light of current evidence, development of PTS is probably multifactorial and is yet incompletely understood as it is still impossible to accurately predict who will end up with PTS. Unfortunately, PTS has a chronic and progressive disease course. Treatment options for established PTS are limited. Compression stockings and frequent limb elevation are the two mostly practiced methods.
Therefore, the main purpose of this study was to assess the severity and associated factors among patients with DVT attending anticoagulation clinics in two government hospitals in Sri Lanka. By assessing the associated factors and patient awareness we will be able to identify lapses in the knowledge and improve awareness about PTS among patients, clinicians, and healthcare workers in anticoagulation clinics.
The study also looked at the efficacy of elastic compression stockings (ECSs) in preventing PTS in patients following acute DVT.
| Materials and Methods | ▴Top |
A descriptive cross-sectional study was conducted to determine the prevalence and associated factors of PTS in DVT patients attending anticoagulation clinics in two government hospitals of Sri Lanka.
Clinics included: 1) Professorial unit anticoagulation clinic at Colombo South Teaching Hospital, Sri Lanka; 2) Anticoagulation clinic at Colombo South Teaching Hospital, Sri Lanka (non-professorial units); and 3) Anticoagulation clinic at Colombo North Teaching Hospital, Sri Lanka.
Inclusion criteria
Both male and female patients above 18 years with DVT, after 6 months and less than 2 years of the acute episode were included in this study.
Exclusion criteria
Those who were studied at < 6 months or > 2 years after the acute DVT were excluded.
Eighty (80) patients who fulfilled inclusion criteria were included in the study. Anthropometric measurements (body weight using an electronic scale, height using measuring tape up to the nearest 0.5 cm) were measured. Privacy of the patient was ensured while obtaining the measurements. Information on duplex ultrasound scan reports at diagnosis and after 3 - 4 months of acute DVT was used to assess residual thrombosis, INR records during the initial 4 months of anticoagulation and D-dimer reports were collected. Each participant was assessed with the Villalta scale to diagnose PTS and its severity. An interviewer-administered questionnaire was used to obtain other necessary information, the demographic details of the person, risk factors, and details of ECS use and awareness of PTS.
Villalta scale (Fig. 1) [12] was applied both as a binary and as a graded scale (0 - 3) to diagnose and determine severity of PTS among the study population. A score of 5 or above was considered diagnostic. Severity was determined using criteria of a score of 5 - 9 as mild PTS, 10 - 14 moderate and 15 or above or presence of a venous ulcer as severe PTS.
Statistical Package for the Social Sciences (SPSS version 23) was used in data analysis. Recorded data were analyzed using paired t-test, Chi-square and analysis of variance (ANOVA) to determine association.
Ethical consideration
Ethical approval was taken from the ethical review committee of Colombo South Teaching Hospital, Kalubowila, Sri Lanka. Permission from the directors and consultants of anticoagulation clinics of relevant hospitals was obtained prior to the access. The anonymity and confidentiality of the data and privacy of the patients were secured by using the clinic number without indicating the name of the person. A complete oral explanation regarding the study, its objectives, how the study would be conducted and what would be expected were provided to the participants. The study was conducted in compliance with the ethical standards of the responsible institutions.
| Results | ▴Top |
Within the study population minimum age recorded was 18 years and the maximum was 74 years, where the majority of them fell within the age group of 45 - 65 years. Mean age of the population was 50.6 years. Majority were females (n = 57, 71.3%) with an approximate male to female ratio of 1: 2.4 (Table 1).
 Click to view | Table 1. Gender Distribution of DVT Patients |
Thirty-six (36) patients (45%) demonstrated the lowest score of 5 or above fulfilling a diagnosis of PTS (Table 2). In the group of diagnosed PTS, majority (n = 28/36, 77.8%) showed mild PTS, five patients had moderate PTS (13.9%) and 8.3% (n = 3) had severe PTS where one patient suffered extreme PTS with debilitating leg ulcers.
Click to view | Table 2. Prevalence of PTS |
Within the study population, recurrent DVT (P = 0.002), higher BMI (P = 0.073) (Table 3) and pre-existing venous incompetence (P = 0.032) demonstrated significant association with PTS. No significant association with gender, age at onset of venous thrombosis or increasing age was noted.
Click to view | Table 3. Association With Age and BMI |
Data also showed a very significant association with residual thrombosis at 3 months (P = 0.001), however, with an associated bias of a very low sample number with a repeat scan at 3 months.
Further, thrombosis in proximal deep veins demonstrated a strong association with PTS (P = 0.002) where 29 (80.6%) patients diagnosed with PTS within the study population being with post-proximal DVT (Table 4). Only seven patients (19.4%) were with post-distal DVT. This observation correlated well with the higher prevalence of PTS (n = 29, 59.2%) among patients who had preceding proximal DVT, and a low prevalence of PTS (n = 7, 22.6%) in those with the distal DVT within the study population. There was no significant association of PTS with unprovoked DVT (Table 5).
Click to view | Table 4. Site vs. PTS Presence |
Click to view | Table 5. Nature of DVT vs. PTS Presence |
Sub therapeutic anticoagulation during the initial face of a DVT was not analyzed as an associated factor for PTS due to lack of consistent follow-up INR recordings on patient records. D-dimer tests were hardly done across all three clinics.
Unfortunately, awareness of this clinical syndrome as a possible long-term complication of DVT was extremely low among the study population (n = 0).
ECS usage post DVT showed significant variation among patients especially the type of ECS, duration they wore during the day and consistency of the practice over the period largely varied. Data obtained were categorized in to three groups, never, less than 6/12 or occasionally or more than 6/12 or regularly (Table 6). Cross analysis of these groups failed to show significant association of use of ECS as a preventive measure (P = 0.61), however with the caveat of observed extreme variable use of ECS and patient bias.
Click to view | Table 6. Stockings vs. PTS presence |
| Discussion | ▴Top |
Prevalence of PTS among the study population was 45%, in keeping with available prevalence data of about 50% from studies done using validated diagnostic criteria [4, 5]. Majority demonstrated mild PTS and 8.3% had severe PTS. Though these rates cannot be directly applied to general population, they reflect a significant disease burden among the post thrombotic patient group in Sri Lanka.
Recurrent DVT, higher BMI, pre-existing venous incompetence, and proximal site of DVT demonstrated a significant association with PTS.
No significant association with gender, age at onset of venous thrombosis or increasing age was noted. Data also showed a very significant association with residual thrombosis at 3 months. These findings were in keeping with current available studies.
A prospective multicenter cohort study done by Khan et al in 387 outpatients and inpatients revealed that venous thrombosis of the common femoral or iliac vein (2.23 increase in score vs. distal (calf) venous thrombosis; P < 0.001), higher BMI (0.14 increase in score per kg/m2; P < 0.001), previous ipsilateral venous thrombosis (1.78 increase in score; P = 0.001) and older age (0.30 increase in score per 10-year age increase; P = 0.011) were significant additional predictors of PTS over the time [20]. Female sex was inconsistently associated with PTS [20, 22].
A prospective study on 111 patients with a diagnosis of DVT of the lower limb looked at noninvasive radiological predictors of PTS. Presence of thrombosis in proximal veins at diagnosis had a higher risk compared with distal thrombosis (risk ratio (RR): 2.3%, 95% confidence interval (CI): 1.0 - 5.6). PTS was diagnosed in 62% of patients with residual thrombosis in the proximal veins after an interval of 6 weeks following DVT, leading to a 1.6-fold increased risk (95% CI: 1.0 - 2.5). Valvular reflux in the superficial veins at 6 weeks following DVT was a predictor with a 1.6-fold increased risk as compared to those without superficial reflux (95% CI: 1.1 - 2.3). The study concluded that age over 50 years, proximal localization of the thrombus at entry, residual proximal thrombosis and superficial valvular reflux at 6 weeks as leading risk factors of PTS in patients with a first episode of DVT. Also, it concluded that duplex scanning after 6 weeks of acute DVT to be an important noninvasive radiological method that can be used for the detection of patients at risk of PTS early [21]. Presence of superficial venous incompetence/varicose veins acts as an independent predictor of subsequent PTS development [24, 25].
As with any health hazard, raising awareness among at-risk group and healthcare professionals plays an important role in prevention of PTS. Unfortunately, knowledge of this clinical syndrome as a possible long-term complication of DVT was extremely low among the study population. PTS-related symptoms get worse on standing and walking. This brings about a major impact on activities of daily living and quality of life of these patients [26-29].
ECSs reduce venous hypertension, improve venous reflux, and thus improve microcirculation [30]. A meta-analysis of two historic studies on the role of ECSs/graduated compression stockings (GCSs) in prevention of PTS; Pradoni et al [31] and Ginsberg et al [32] concluded that sustained use of ECS following a DVT to be effective in lowering the risk of PTS. However, SOX trial, a Canadian multicenter double-blinded placebo-controlled trial of ECS efficacy in preventing PTS studied 806 patients (410 patients were randomly assigned to active ECS and 396 to placebo ECS). The cumulative incidence of PTS was 14.2% in active ECS versus 12.7% in placebo ECS (hazard ratio adjusted for center: 1.13, 95% CI: 0.73 - 1.76; P = 0.58). The study concluded that ECS did not prevent PTS after first proximal DVT [33]. In accordance, ACCP guidelines on anti-thrombotic therapy and prevention of thrombosis (2016 revision) no longer recommends the routine use of ECS for the prevention of PTS in patients with DVT [34]. In the study conducted by Kahn et al, a comparison between Villalta scale and other score systems showed that the proportion of patients labeled as having PTS (37%) was nearly five times more than that with Ginsberg measure, indicating that Ginsberg has a tendency to overlook mild PTS [35]. SOX trial used Ginsberg criteria to diagnose PTS which could have overlooked mild cases of PTS, which would possibly explain the wide variation of study out comes on this setting. Determination of the role of ECS in unselected/high-risk patient groups would provide a better understanding on its role in PTS prevention.
We were unable to reliably conclude on the role of ECS as a preventative method of PTS given the wide variation of its use among the study population; however, it was apparent that use of ECS in this setting to be less practical and poorly adhered by the patient.
Conclusions
The study showed a significant prevalence of PTS among patients with previous DVT. High BMI, proximal site of the DVT, residual thrombosis and pre-existing venous incompetence demonstrated a significant association with PTS. In the light of current evidence, development of PTS is probably multifactorial, and the awareness of this debilitating long-term complication of DVT appears to be extremely low among patients. There is clearly a hidden but significant health care and socio-economic burden associated with PTS.
A validated risk assessment tool should be used to identify at-risk patients as prevention appears to be the best approach to this irreversible morbidity. SOX-PTS score, an externally validated clinical score should be incorporated into the initial assessment to identify at-risk patients. Raising awareness and modifying risk factors associated with PTS should be emphasized and should be made an essential aspect in DVT management to improve long-term outcomes.
Acknowledgments
The authors would like to thank Dr Nishadhya Ranasinghe, Consultant Hematologist, Colombo South Teaching Hospital, Sri Lanka and Dr Yasintha Costa, Consultant Hematologist, Colombo North Teaching Hospital Sri Lanka.
Financial Disclosure
No funding sources to declare.
Conflict of Interest
The authors declare no conflict of interest.
Informed Consent
Informed written consent was obtained from each participant before the commencement of the study.
Author Contributions
SA wrote the proposal, managed the literature survey, carried out the data collection, performed data analysis and wrote the first draft of the manuscript. IW and CK designed the study, corrected the proposal and literature survey, supervised and guided methodology and data analysis and corrected and modified the manuscript. All the authors read and approved the final version of the manuscript.
Data Availability
Any inquiries regarding supporting data availability of this study should be directed to the corresponding author.
Abbreviations
PTS: post-thrombotic syndrome; DVT: deep vein thrombosis; BMI: body mass index; ISTH: International Society of Thrombosis and Hemostasis; ECS: elastic compression stocking
| References | ▴Top |
- Eklof B, Perrin M, Delis KT, Rutherford RB, Gloviczki P, American Venous F, European Venous F, et al. Updated terminology of chronic venous disorders: the VEIN-TERM transatlantic interdisciplinary consensus document. J Vasc Surg. 2009;49(2):498-501.
doi pubmed - Brandjes DP, Buller HR, Heijboer H, Huisman MV, de Rijk M, Jagt H, ten Cate JW. Randomised trial of effect of compression stockings in patients with symptomatic proximal-vein thrombosis. Lancet. 1997;349(9054):759-762.
doi - Kakkar VV, Lawrence D. Haemodynamic and clinical assessment after therapy for acute deep vein thrombosis. Am J Surg. 1985;150:54-63.
- Gabriel F, Labios M, Portoles O, Guillen M, Corella D, Frances F, Martinez M, et al. Incidence of post-thrombotic syndrome and its association with various risk factors in a cohort of Spanish patients after one year of follow-up following acute deep venous thrombosis. Thromb Haemost. 2004;92(2):328-336.
doi pubmed - Roumen-Klappe EM, den Heijer M, Janssen MC, van der Vleuten C, Thien T, Wollersheim H. The post-thrombotic syndrome: incidence and prognostic value of non-invasive venous examinations in a six-year follow-up study. Thromb Haemost. 2005;94(4):825-830.
doi pubmed - Mohr DN, Silverstein MD, Heit JA, Petterson TM, O'Fallon WM, Melton LJ. The venous stasis syndrome after deep venous thrombosis or pulmonary embolism: a population-based study. Mayo Clin Proc. 2000;75(12):1249-1256.
doi pubmed - Kahn SR, Ginsberg JS. The post-thrombotic syndrome: current knowledge, controversies, and directions for future research. Blood Rev. 2002;16(3):155-165.
doi - Hopkins NF, Wolfe JH. ABC of vascular diseases. Deep venous insufficiency and occlusion. BMJ. 1992;304(6819):107-110.
doi pubmed - Kahn SR, Ginsberg JS. Relationship between deep venous thrombosis and the postthrombotic syndrome. Arch Intern Med. 2004;164(1):17-26.
doi pubmed - Prandoni P, Kahn SR. Post-thrombotic syndrome: prevalence, prognostication and need for progress. Br J Haematol. 2009;145(3):286-295.
doi pubmed - Widmer L, Da Silva A, Madar G. Varikosis und chronisch venose Insuffizienz [Varicosis and chronic venous insufficiency]. Venen-, Arterien-, Krankheiten, koronare Herzkrankheit bei Berufstatigen. Easier Srudie 1-111. In: Widmer LK, Stahelin HB, Nissen C, da Silva A, editors. Verlag Hans Huber, Bern. 1981.
- Villalta S, Bagatella P, Piccioli A, Lensing AWA, Prins MH, Prandoni P. Assessment of validity and reproducibility of a clinical scale for the post-thrombotic syndrome. Haemostasis. 1994;24:158a.
- Ginsberg JS, Turkstra F, Buller HR, MacKinnon B, Magier D, Hirsh J. Postthrombotic syndrome after hip or knee arthroplasty: a cross-sectional study. Arch Intern Med. 2000;160(5):669-672.
doi pubmed - Porter JM, Moneta GL. Reporting standards in venous disease: an update. International Consensus Committee on Chronic Venous Disease. J Vasc Surg. 1995;21(4):635-645.
doi - Rutherford RB, Padberg FT, Jr., Comerota AJ, Kistner RL, Meissner MH, Moneta GL. Venous severity scoring: An adjunct to venous outcome assessment. J Vasc Surg. 2000;31(6):1307-1312.
doi pubmed - Kolbach DN, Neumann HA, Prins MH. Definition of the post-thrombotic syndrome, differences between existing classifications. Eur J Vasc Endovasc Surg. 2005;30(4):404-414.
doi pubmed - Kahn SR, Partsch H, Vedantham S, Prandoni P, Kearon C, Subcommittee on Control of Anticoagulation of the S, Standardization Committee of the International Society on T, et al. Definition of post-thrombotic syndrome of the leg for use in clinical investigations: a recommendation for standardization. J Thromb Haemost. 2009;7(5):879-883.
doi pubmed - Kahn SR. Measurement properties of the Villalta scale to define and classify the severity of the post-thrombotic syndrome. J Thromb Haemost. 2009;7(5):884-888.
doi pubmed - Chitsike RS, Rodger MA, Kovacs MJ, Betancourt MT, Wells PS, Anderson DR, Chagnon I, et al. Risk of post-thrombotic syndrome after subtherapeutic warfarin anticoagulation for a first unprovoked deep vein thrombosis: results from the REVERSE study. J Thromb Haemost. 2012;10(10):2039-2044.
doi pubmed - Kahn SR, Shrier I, Julian JA, Ducruet T, Arsenault L, Miron MJ, Roussin A, et al. Determinants and time course of the postthrombotic syndrome after acute deep venous thrombosis. Ann Intern Med. 2008;149(10):698-707.
doi pubmed - Tick LW, Doggen CJ, Rosendaal FR, Faber WR, Bousema MT, Mackaay AJ, P VANB, et al. Predictors of the post-thrombotic syndrome with non-invasive venous examinations in patients 6 weeks after a first episode of deep vein thrombosis. J Thromb Haemost. 2010;8(12):2685-2692.
doi pubmed - Stain M, Schonauer V, Minar E, Bialonczyk C, Hirschl M, Weltermann A, Kyrle PA, et al. The post-thrombotic syndrome: risk factors and impact on the course of thrombotic disease. J Thromb Haemost. 2005;3(12):2671-2676.
doi pubmed - Latella J, Desmarais S, Kahn S, Veto I. The relationship between D-dimer level, venous valvularreflux and development of the post-thrombotic syndrome after deep venous thrombosis [abstract]. Blood. 2008;112(11):1821.
doi - Wille-Jorgensen P, Jorgensen T, Andersen M, Kirchhoff M. Postphlebitic syndrome and general surgery: an epidemiologic investigation. Angiology. 1991;42(5):397-403.
doi pubmed - Ashrani AA, Heit JA, Lahr BD, et al. Role of venous outflow obstruction and venous valvular incompetence as mechanisms for venous stasis syndrome following deep vein thrombosis: a population-based cohort study. Blood. 2006;108:1495.
doi - Kahn SR, Hirsch A, Shrier I. Effect of postthrombotic syndrome on health-related quality of life after deep venous thrombosis. Arch Intern Med. 2002;162(10):1144-1148.
doi pubmed - Kahn SR, Shbaklo H, Lamping DL, Holcroft CA, Shrier I, Miron MJ, Roussin A, et al. Determinants of health-related quality of life during the 2 years following deep vein thrombosis. J Thromb Haemost. 2008;6(7):1105-1112.
doi pubmed - Ashrani AA, Silverstein MD, Rooke TW, Lahr BD, Petterson TM, Bailey KR, Melton LJ, 3rd, et al. Impact of venous thromboembolism, venous stasis syndrome, venous outflow obstruction and venous valvular incompetence on quality of life and activities of daily living: a nested case-control study. Vasc Med. 2010;15(5):387-397.
doi pubmed - Ramacciotti E, Gomes M, de Aguiar ET, Caiafa JS, de Moura LK, Araujo GR, Truzzi A, et al. A cost analysis of the treatment of patients with post-thrombotic syndrome in Brazil. Thromb Res. 2006;118(6):699-704.
doi pubmed - Pierson S, Pierson D, Swallow R, Johnson G, Jr. Efficacy of graded elastic compression in the lower leg. JAMA. 1983;249(2):242-243.
doi pubmed - Prandoni P, Lensing AW, Prins MH, Frulla M, Marchiori A, Bernardi E, Tormene D, et al. Below-knee elastic compression stockings to prevent the post-thrombotic syndrome: a randomized, controlled trial. Ann Intern Med. 2004;141(4):249-256.
doi pubmed - Ginsberg JS, Magier D, Mackinnon B, Gent M, Hirsh J. Intermittent compression units for severe post-phlebitic syndrome: a randomized crossover study. CMAJ. 1999;160(9):1303-1306.
doi - Kahn SR, Shbaklo H, Shapiro S, Wells PS, Kovacs MJ, Rodger MA, Anderson DR, et al. Effectiveness of compression stockings to prevent the post-thrombotic syndrome (the SOX Trial and Bio-SOX biomarker substudy): a randomized controlled trial. BMC Cardiovasc Disord. 2007;7:21.
doi pubmed - Kearon C, Akl EA, Ornelas J, Blaivas A, Jimenez D, Bounameaux H, Huisman M, et al. Antithrombotic therapy for VTE disease: CHEST guideline and expert panel report. Chest. 2016;149(2):315-352.
doi pubmed - Kahn SR, Desmarais S, Ducruet T, Arsenault L, Ginsberg JS. Comparison of the Villalta and Ginsberg clinical scales to diagnose the post-thrombotic syndrome: correlation with patient-reported disease burden and venous valvular reflux. J Thromb Haemost. 2006;4(4):907-908.
doi pubmed
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Current Surgery is published by Elmer Press Inc.