

| Journal of Current Surgery, ISSN 1927-1298 print, 1927-1301 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Curr Surg and Elmer Press Inc |
| Journal website https://www.currentsurgery.org |
Original Article
Volume 13, Number 1, September 2023, pages 1-5

Remimazolam as an Adjunct to General Anesthesia During Spine Surgery in Adolescents
Mitchell Hughesa, Shelby Corneliusa, Allen Kadadob, Reid Chambersb, Brian Hallc, Joseph D. Tobiasc, d, e
aHeritage College of Osteopathic Medicine - Dublin Campus, Dublin, Ohio and Ohio University, Athens, OH, USA
bDepartment of Pediatric Orthopedic Surgery, Nationwide Children’s Hospital and The Ohio State University, Columbus, OH, USA
cDepartment of Anesthesiology & Pain Medicine, Nationwide Children’s Hospital, Columbus, OH, USA
dDepartment of Anesthesiology & Pain Medicine, The Ohio State University College of Medicine, Columbus, OH, USA
eCorresponding Author: Joseph D. Tobias, Department of Anesthesiology & Pain Medicine, Nationwide Children’s Hospital, Columbus, OH 43205, USA
Manuscript submitted July 6, 2023, accepted August 30, 2023, published online September 30, 2023
Short title: Remimazolam and Spine Surgery
doi: https://doi.org/10.14740/jcs472
| Abstract | ▴Top |
Background: Remimazolam is a benzodiazepine that has recently been released for clinical use. Similar to midazolam, it has sedative, anxiolytic, and amnestic properties. However, its metabolism is different as it undergoes metabolism by tissue esterases with a half-life of 5 - 10 min and a limited context-sensitive half-life.
Methods: We retrospectively reviewed our experience with the use of remimazolam as an adjunctive to general anesthesia during spine surgery.
Results: The study cohort included 40 patients, ranging in age from 11 to 35 years and in weight from 21 to 126 kg. Remimazolam was added as an adjunct to maintenance anesthesia with propofol, desflurane, or dexmedetomidine/ketamine at a starting dose of 2.5 - 10 µg/kg/min (median dose 5 µg/kg/min). Maintenance doses ranged from 1.5 to 30 µg/kg/min (median dose 8 µg/kg/min). Remimazolam was infused for an average of 5.1 h per patient or a total of 203 h of infusion in the 40 patients. With the infusion of remimazolam, the requirements for the volatile agent or propofol were decreased by approximately 40-50%. No adverse effects related to remimazolam were noted.
Conclusions: Remimazolam is an effective adjunct to general anesthesia during spinal surgery, resulting in a significant decrease in requirements for propofol or volatile anesthetic agents.
Keywords: Remimazolam; Neurophysiological monitoring; Posterior spinal fusion; General anesthesia; Benzodiazepine
| Introduction | ▴Top |
Remimazolam is an ester metabolized derivative of the intravenous benzodiazepine, midazolam [1, 2]. It received FDA approval for use in adults in 2020. Its sedative, anxiolytic, and amnestic properties are similar to other benzodiazepines including midazolam. However, it has a novel metabolic pathway with ester hydrolysis providing a half-life of 5 - 10 min and a limited context-sensitive half-life. Preliminary clinical experience has demonstrated its efficacy in the adult population as a primary agent for procedural sedation or as an adjunct to general anesthesia [3-6]. To date, there are limited data regarding the use of remimazolam in pediatric-aged patients. We present our preliminary experience using remimazolam as an adjunct to general anesthesia during spinal surgery in children and adolescents.
| Materials and Methods | ▴Top |
This retrospective study was reviewed and approved by the IRB of Nationwide Children’s Hospital (Columbus, Ohio) and conducted in accordance with the guidelines of the Declaration of Helsinki. Given the retrospective nature of the study, the need for individual written informed consent was waived. Patient confidentiality was maintained by the use of deidentified data and storage of data in a secure location on a password-protected network. Access to data was available only to collaborators directly involved in the study.
In January 2022, remimazolam was added to the operating room formulary with initial use restricted to patients ≥ 10 years of age and ≥ 40 kg in weight. From the hospital-based pharmacy database, patients presenting for anesthetic care during spinal surgery who received a continuous intraoperative remimazolam infusion as an adjunct to either total intravenous anesthesia (TIVA) or a volatile anesthesia-based technique with desflurane were identified and included in subsequent analysis.
We utilized our previously published departmental practice pathway for intraoperative anesthetic care during posterior spinal fusion including neurophysiological monitoring with motor-evoked potentials (MEPs) and somatosensory-evoked potentials [7]. Preoperative medications included placement of a scopolamine patch and the oral administration of aprepitant (40 mg) as prophylaxis against postoperative nausea and vomiting (PONV). Oral gabapentin was administered as an adjunct to postoperative analgesia. Anesthetic induction was accomplished by the inhalation of sevoflurane or the administration of intravenous propofol. Following anesthetic induction, a neuromuscular blocking agent (rocuronium 0.2 - 0.3 mg/kg) was administered to facilitate endotracheal intubation. Two peripheral intravenous cannulas and an arterial cannula were then placed. Maintenance anesthesia consisted of inhaled desflurane, adjusted to maintain the bispectral index (BIS) at 40 - 60 to ensure amnesia. Methadone (0.1 mg/kg) and an opioid infusion (remifentanil or sufentanil) were then administered. The opioid infusion was adjusted to maintain the mean arterial pressure (MAP) at 55 - 65 mm Hg. Clevidipine or labetalol was administered as needed as adjuncts for MAP control. Blood avoidance techniques included control of the MAP, intraoperative blood salvage, and the administration of tranexamic acid. Acetaminophen (15 mg/kg up to 1 g) was administered intraoperatively as an adjunct to postoperative analgesia. Additional prophylaxis against PONV included intravenous ondansetron (4 mg) and dexamethasone (8 mg).
For intraoperative administration, remimazolam was prepared according to the manufacturer’s recommendation from a lyophilized powder. It was diluted in normal saline to a final concentration of 20 mg/8 mL (2.5 mg/mL) and provided to the anesthetic providers in a syringe. Intraoperatively, the medication was administered by an infusion pump. Our dosing preference of using µg/kg/min and not mg/kg/h was determined based on our usual intraoperative practice for the majority of continuous intravenous infusions. Based on dosing information from the adult literature (mg/h), we extrapolated weight-based dosing with recommendations for a bolus dose of 50 - 200 µg/kg (maximum of 5 mg) and an infusion starting at 3 - 5 µg/kg/min with an increase up to 30 µg/kg/min as needed.
Demographic data included age, weight, body mass index, associated comorbid conditions, and gender. Intraoperative information collected included the surgical procedure, surgical duration, anesthetic and sedative agents used, their dose, and mode of administration (continuous or intermittent). Intraoperative and postoperative adverse effects including hypotension, bradycardia, respiratory arrest, apnea, or hypoventilation were identified. Additional information regarding intraoperative adverse effects was identified by the need for rescue medications. The latter included anticholinergic agents or vasoactive agents (epinephrine, phenylephrine, vasopressin, or ephedrine). Information regarding remimazolam was identified and collected including its starting dose, average maintenance dose, changes in dosing during the intraoperative period, and duration of the infusion. The electronic medical record was also reviewed for adverse effects that could be specifically identified related to remimazolam by noting any temporary pauses in the infusion or decreases in the infusion rate that coincided with adverse hemodynamic effects. Efficacy was determined by a review of data from intraoperative depth of anesthesia monitors (BSI) when available, as well as the dosing requirements for adjunctive sedative and analgesic agents. Descriptive study statistics for this retrospective study include the number, mean ± standard deviation (SD), and range.
| Results | ▴Top |
The study cohort included 40 patients presenting for posterior spinal fusion to treat idiopathic or neuromuscular scoliosis. The patients ranged in age from 11 to 35 years (mean 15.3 ± 4.2 years) and in weight from 21 to 126 kg (mean 55.2 ± 21.1 kg). There were 11 male and 29 female patients. The primary technique for general anesthesia included a volatile agent-based technique in 27 patients (desflurane in 26 patients and sevoflurane in one patient) and TIVA in 13 patients, 11 of whom received propofol as the primary agent while two received a combination of ketamine and dexmedetomidine. The maintenance anesthesia (volatile-based or TIVA) included a continuous opioid infusion with sufentanil (17 patients), remifentanil (22 patients), or both sufentanil and remifentanil (one patient) over the course of their procedure. Additionally, 39 of the 40 patients received a single intraoperative dose of methadone (0.1 - 0.15 mg/kg).
All 40 patients also received remimazolam with a starting dose ranging from 2.5 to 10 µg/kg/min (median dose 5 µg/kg/min). Maintenance doses of remimazolam ranged from 1.5 to 30 µg/kg/min (median dose 8 µg/kg/min). The differences in the initial infusion rates, maintenance infusion rates, and overall infusion rates of remimazolam in all 40 patients are outlined in Table 1. Remimazolam was infused for an average of 5.1 h per patient (range 2.6 to 9.13 h) for a total of 203 h of infusion in the 40 patients. The differences in the initial infusion rate and maintenance infusion rates between the volatile-based, propofol-based, and dexmedetomidine-ketamine-based techniques are outlined in Table 2. The depth of anesthesia was monitored by the BIS and the volatile agent or propofol was adjusted to maintain the BIS at 40 - 60. With the infusion of the remimazolam, the inspired concentration of the volatile agent was decreased from a starting value of 3.5-4% to 2-2.6% and the propofol infusion was decreased from a starting infusion rate of 150 - 200 to 70 - 100 µg/kg/min.
 Click to view | Table 1. Remimazolam Infusion Rates (µg/kg/min) |
Click to view | Table 2. Remimazolam Infusion Rates based on Anesthetic Technique (µg/kg/min) |
No patients experienced adverse hemodynamic effects related to remimazolam, no downward titration of the infusion was required due to adverse effects, and no vasoactive agents were administered to treat hemodynamic effects that were primarily related to the remimazolam infusion. No patients received anticholinergic agents. Although three patients received epinephrine, three received norepinephrine, 29 received phenylephrine, and two patients received vasopressin; none of these medications were given to treat hemodynamic adverse effects related to remimazolam but to treat hypotension related to blood loss and other intraoperative events. Additional intraoperative medications administered are noted in Figure 1.
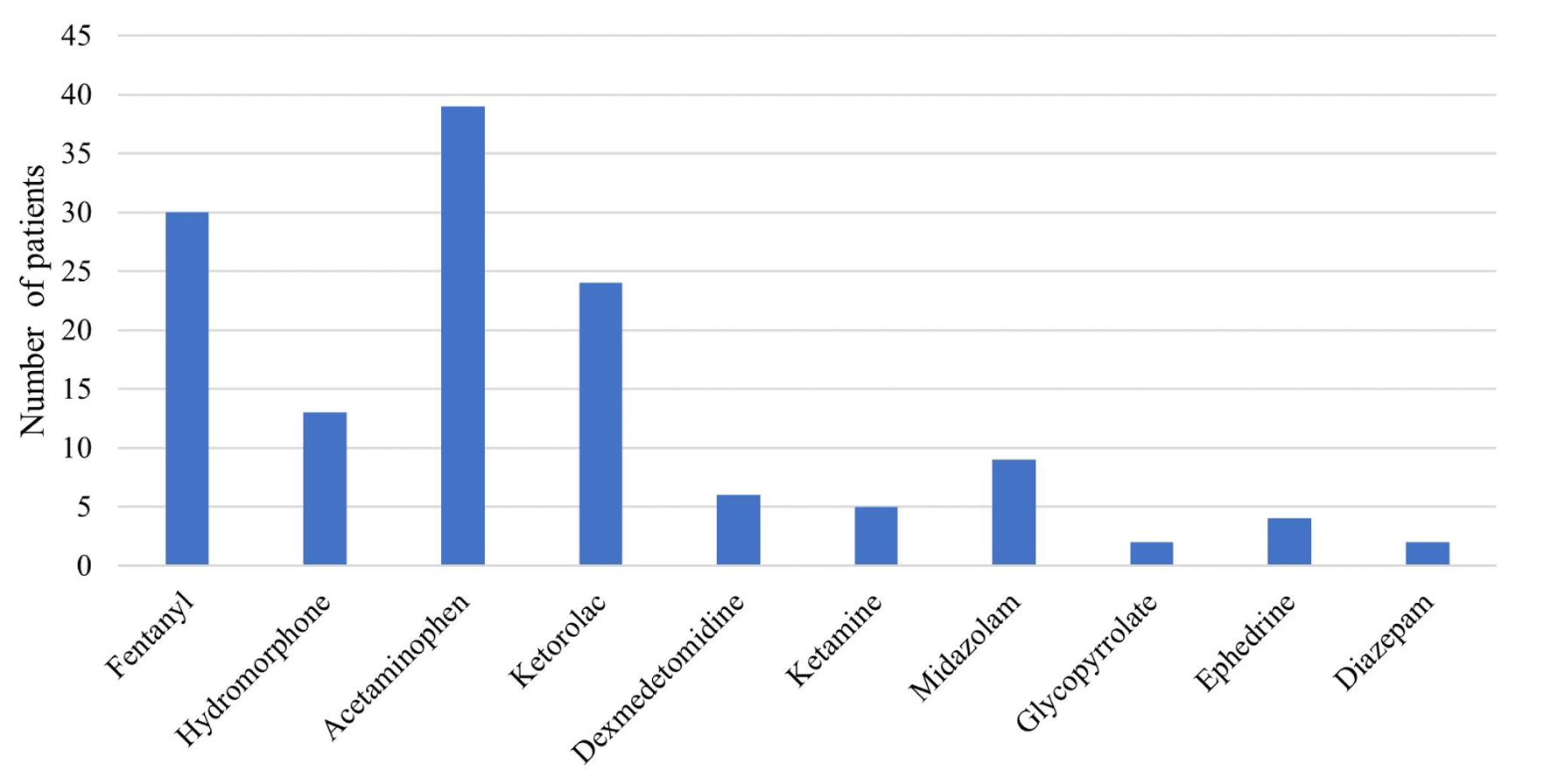 Click for large image | Figure 1. Additional intraoperative medications administered to the patients in the study cohort. The x-axis lists the medication and the y-axis shows the number of patients from the cohort of 40 that received each medication. |
| Discussion | ▴Top |
Our preliminary experience demonstrates that remimazolam is an effective adjunct to general anesthesia with either a volatile agent or TIVA during spine surgery. In our cohort of patients, starting doses generally ranged from 1.5 to 30 µg/kg/min with a median maintenance infusion rate of 6 µg/kg/min. With the use of remimazolam as an adjunct to general anesthesia, the requirements for the volatile agent (desflurane) or propofol were decreased by approximately 25-30% [7, 8]. The lower dose requirements for either the volatile agent or propofol may mitigate some of the concerns of these agents that are routinely used for maintenance anesthesia during spine surgery including effects on neurophysiological monitoring (volatile agents) or prolonged awakening due to context-sensitive half-life (propofol), which may impact rapid recovery from anesthesia which may be necessary to when a wakeup is needed intraoperatively or to ensure intact neurologic function at the completion of the surgical procedure [9-12]. Additionally, our anecdotal experience demonstrates no clinically significant impact on neurophysiologic monitoring including elicitation of MEPs and in fact, subjectively improved monitoring when combined with a volatile-based technique as it allows a reduction in the expired concentration of desflurane required to maintain general anesthesia as assessed by the BIS.
Preliminary clinical data with remimazolam have demonstrated it to be effective in providing procedural sedation in adults during invasive bronchoscopy as well as upper and lower gastrointestinal endoscopy [13-15]. During these invasive procedures, remimazolam by bolus dosing or continuous infusion, has been shown to have an efficacy similar to that of propofol with a limited adverse effect profile. Beneficial physiologic effects include a limited impact on hemodynamic function, no pain with intravenous administration, a reduction of nausea and vomiting following the procedure, and a rapid return to baseline neurologic function when administration is discontinued [16]. In addition to its use as the primary agent for procedural sedation, remimazolam has been shown to be an effective primary agent or adjunct to general anesthesia in adults [17-19]. To date, reports regarding the use of remimazolam in pediatric-aged patients have included only anecdotal retrospective experiences from single case reports or small case series [20-26].
Two previous case reports have outlined the use of remimazolam during neurophysiologic monitoring for spinal fusion [21, 27]. Kamata et al presented anecdotal experience with a combination of remimazolam and remifentanil for TIVA during PSF in a 12-year-old girl with an egg allergy which led to the author’s use of remimazolam instead of propofol [21]. Effective MEPs were obtained during TIVA with remimazolam at 0.9 mg/kg/h and remifentanil at 0.35 µg/kg/min. A similar experience was reported by Kondo et al with intraoperative MEP monitoring during spinal fusion in two adult patients (70 and 76 years of age) [27]. Intraoperative dosing for case 1 included remimazolam at 0.5 mg/kg/h and remifentanil at 0.2 µg/kg/min. In the second case, remifentanil was infused at 0.3 µg/kg/min; however, a higher dose of remimazolam was required. The remimazolam infusion was increased from 0.5 to 1.5 mg/kg/h with no impact on the MEP signals. In these two cases, the remimazolam infusion was titrated to achieve a BSI of 40 - 60. The authors concluded that TIVA with infusions of remimazolam and remifentanil was a viable option to provide intraoperative anesthesia during spine surgery with MEP monitoring.
Limitations of our current study include its retrospective nature which may result in difficulties with accurate identification of all confounding variables. The design may have limited the identification of adverse hemodynamics to those that could be identified by the need to adjust the infusion rate or pause its administration. While vasoactive agents were occasionally administered, causality cannot be ascribed to anesthetic agents alone, as adjustments to hemodynamics are commonly requested during posterior spinal fusion secondary to intraoperative changes in neuromonitoring or specific portions of the procedure. Additionally, without a prospective design and a control group, the delineation of true outcome data including the impact of remimazolam on volatile agent propofol dosing is limited. Finally, given the nature of our clinical patient population and the retrospective design, there was heterogeneity in the demographics (age and weight) of study cohort as well as the associated co-morbid conditions.
In adults for procedural sedation and intraoperative care, dosing regimens for remimazolam have included intermittent bolus dosing, bolus dosing followed by a continuous infusion or a continuous infusion alone. Remimazolam has been used as the sole agent for procedural sedation and as a supplement to volatile anesthetic agents during general anesthesia. In these clinical scenarios, the infusions, titrated to clinical effect, have varied from 1 to 2 mg/kg/h. These latter dosing ranges are similar to the dosing range used in our current cohort of patients. For our cases, the medication was administered by a syringe-based infusion pump through a separate intravenous site to avoid drug incompatibilities. In our clinical practice, dosing was calculated as µg/kg/min and not mg/kg/h.
In summary, remimazolam is an ultra-short acting benzodiazepine, approved in 2020 by the FDA for procedural sedation in adults. Although there is accumulating clinical experience with its use in pediatric-aged patients, it does not hold FDA approval for use in children. Our preliminary clinical experience demonstrates its utility as an adjunct to general anesthesia during posterior spinal fusion. There are several additional ongoing studies registered at clinicaltrials.gov describing prospective trials regarding the use remimazolam in various clinical scenarios in pediatric-aged patients. These may provide additional information regarding clinical utility, efficacy, safety, and dosing regimens in children and adolescents. Future prospective studies with demographic and surgical site matched procedures are needed to further define intraoperative dosing requirement, impact on volatile agent and propofol requirements, and effects on neurophysiologic monitoring.
Acknowledgments
None to declare.
Financial Disclosure
None to declare.
Conflict of Interest
None to declare.
Informed Consent
Given the retrospective nature of the study, the need for individual written informed consent was waived.
Author Contributions
MH, SC: chart review and preparation of manuscript; RC, AK, BH provided clinical care of the patients and review of the final manuscript; JDT: clinical care, manuscript preparation, review, and editing.
Data Availability
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
| References | ▴Top |
- Lee A, Shirley M. Remimazolam: a review in procedural sedation. Drugs. 2021;81(10):1193-1201.
doi pubmed - Kim KM. Remimazolam: pharmacological characteristics and clinical applications in anesthesiology. Anesth Pain Med (Seoul). 2022;17(1):1-11.
doi pubmed pmc - Morimoto Y. Efficacy and safety profile of remimazolam for sedation in adults undergoing short surgical procedures. Ther Clin Risk Manag. 2022;18:95-100.
doi pubmed pmc - Xiao X, Xiao N, Zeng F, Chen H, Zhang L, He X. Gastroscopy sedation: clinical trial comparing propofol and sufentanil with or without remimazolam. Minerva Anestesiol. 2022;88(4):223-229.
doi pubmed - Hari Y, Satomi S, Murakami C, Narasaki S, Morio A, Kato T, Tsutsumi YM, et al. Remimazolam decreased the incidence of early postoperative nausea and vomiting compared to desflurane after laparoscopic gynecological surgery. J Anesth. 2022;36(2):265-269.
doi pubmed - Sato T, Nishiwaki K. Comparison of remimazolam and propofol in anesthetic management for awake craniotomy: a retrospective study. J Anesth. 2022;36(1):152-155.
doi pubmed - Martin DP, Bhalla T, Thung A, Rice J, Beebe A, Samora W, Klamar J, et al. A preliminary study of volatile agents or total intravenous anesthesia for neurophysiological monitoring during posterior spinal fusion in adolescents with idiopathic scoliosis. Spine (Phila Pa 1976). 2014;39(22):E1318-1324.
doi pubmed - Ngwenyama NE, Anderson J, Hoernschemeyer DG, Tobias JD. Effects of dexmedetomidine on propofol and remifentanil infusion rates during total intravenous anesthesia for spine surgery in adolescents. Paediatr Anaesth. 2008;18(12):1190-1195.
doi pubmed - Hall JE, Levine CR, Sudhir KG. Intraoperative awakening to monitor spinal cord function during Harrington instrumentation and spine fusion. Description of procedure and report of three cases. J Bone Joint Surg Am. 1978;60(4):533-536.
pubmed - Tobias JD, Hoernschemeyer DG, Anderson JT. Ankle clonus and wakeup tests during posterior spinal fusion: correlation with bispectral index. Am J Orthop (Belle Mead NJ). 2009;38(4):E75-77.
pubmed - Padberg AM, Bridwell KH. Spinal cord monitoring: current state of the art. Orthop Clin North Am. 1999;30(3):407-433.
doi pubmed - Assessment: intraoperative neurophysiology. Report of the therapeutics and technology assessment subcommittee of the American Academy of Neurology. Neurology. 1990;40(11):1644-1646.
pubmed - Chen S, Wang J, Xu X, Huang Y, Xue S, Wu A, Jin X, et al. The efficacy and safety of remimazolam tosylate versus propofol in patients undergoing colonoscopy: a multicentered, randomized, positive-controlled, phase III clinical trial. Am J Transl Res. 2020;12(8):4594-4603.
pubmed pmc - Chen SH, Yuan TM, Zhang J, Bai H, Tian M, Pan CX, Bao HG, et al. Remimazolam tosilate in upper gastrointestinal endoscopy: A multicenter, randomized, non-inferiority, phase III trial. J Gastroenterol Hepatol. 2021;36(2):474-481.
doi pubmed - Pastis NJ, Yarmus LB, Schippers F, Ostroff R, Chen A, Akulian J, Wahidi M, et al. Safety and efficacy of remimazolam compared with placebo and midazolam for moderate sedation during bronchoscopy. Chest. 2019;155(1):137-146.
doi pubmed - Zhang J, Cairen Z, Shi L, Pang S, Shao Y, Wang Y, Lu Z. Remimazolam versus propofol for procedural sedation and anesthesia: a systemic review and meta-analysis. Minerva Anestesiol. 2022;88(12):1035-1042.
doi pubmed - Mao Y, Guo J, Yuan J, Zhao E, Yang J. Quality of recovery after general anesthesia with remimazolam in patients' undergoing urologic surgery: a randomized controlled trial comparing remimazolam with propofol. Drug Des Devel Ther. 2022;16:1199-1209.
doi pubmed pmc - Doi M, Hirata N, Suzuki T, Morisaki H, Morimatsu H, Sakamoto A. Safety and efficacy of remimazolam in induction and maintenance of general anesthesia in high-risk surgical patients (ASA Class III): results of a multicenter, randomized, double-blind, parallel-group comparative trial. J Anesth. 2020;34(4):491-501.
doi pubmed - Doi M, Morita K, Takeda J, Sakamoto A, Yamakage M, Suzuki T. Efficacy and safety of remimazolam versus propofol for general anesthesia: a multicenter, single-blind, randomized, parallel-group, phase IIb/III trial. J Anesth. 2020;34(4):543-553.
doi pubmed - Horikoshi Y, Kuratani N, Tateno K, Hoshijima H, Nakamura T, Mieda T, Doi K, et al. Anesthetic management with remimazolam for a pediatric patient with Duchenne muscular dystrophy. Medicine (Baltimore). 2021;100(49):e28209.
doi pubmed pmc - Kamata K, Asagi S, Shimoda Y, Kanamori M, Abe N, Sugino S, Tominaga T, et al. Successful recording of direct cortical motor-evoked potential from a pediatric patient under remimazolam anesthesia: a case report. JA Clin Rep. 2022;8(1):66.
doi pubmed pmc - Petkus H, Willer BL, Tobias JD. Remimazolam in a pediatric patient with a suspected family history of malignant hyperthermia. J Med Cases. 2022;13(8):386-390.
doi pubmed pmc - Gyurgyik N, Warren J, Miketic R, Tobias JD. Use of remimazolam as an adjunct to general anesthesia for an adolescent with MELAS syndrome. Pediatr Anesth Crit Care J. 2022;10:49-55.
- Garrett A, Flowers J, Ng V, Tobias JD. Remimazolam for sedation during upper gastrointestinal endoscopy in an adolescent. J Med Cases. 2022;13(10):495-498.
doi pubmed pmc - Kalsotra S, Khan S, McKee C, Tobias JD. Remimazolam as the primary agent for sedation during cardiac catheterization in three patients with comorbid cardiac conduction abnormalities. Cardiol Res. 2023;14(1):86-90.
doi pubmed pmc - Yeh J, McKee C, Chenault K, Tobias JD. Remimazolam as a primary agent for brief invasive and noninvasive procedures: a case series. J Clin Med Res. 2023;15(3):174-180.
doi pubmed pmc - Kondo T, Toyota Y, Narasaki S, Watanabe T, Miyoshi H, Saeki N, Tsutsumi YM. Intraoperative responses of motor evoked potentials to the novel intravenous anesthetic remimazolam during spine surgery: a report of two cases. JA Clin Rep. 2020;6(1):97.
doi pubmed pmc
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Current Surgery is published by Elmer Press Inc.