

| Journal of Current Surgery, ISSN 1927-1298 print, 1927-1301 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Curr Surg and Elmer Press Inc |
| Journal website http://www.currentsurgery.org |
Case Report
Volume 8, Number 1-2, June 2018, pages 22-24
A Rare Presentation of Meckel’s Diverticulum: A Case Report
Naif Almalkia, c, Turki Almalkib
aCollage of Medicine, Taif University, Al Kharj, Saudi Arabia
bCollege of Medicine, Prince Sattam Abdulaziz University, Al Kharj, Saudi Arabia
cCorresponding Author: Turki Almalk, College of Medicine, Prince Sattam Abdulaziz University, Al Kharj, Saudi Arabia
Manuscript submitted January 3, 2018, accepted January 23, 2018
Short title: A Rare Presentation of Meckel’s Diverticulum
doi: https://doi.org/10.14740/jcs335w
| Abstract | ▴Top |
The purpose of this report is to present a rare presentation of Meckel’s diverticulum. A 25-year-old Saudi male was referred to our hospital with recurrent intestinal obstruction; computed tomography was done, which showed distended small bowel. Operative management was discussed with the patient and consent was taken for laparoscopy and laprotomy if indicted. Initially we started with laparoscopy but due to sever distention of bowls and adhesion, midline incision was done and multiple adhesions were released from ascending colon and distal small bowl until it was revealed that he had Meckel’s diverticulum with severe adhesion around.
Keywords: Meckle’s diverticulum; Case report; Rare presentation
| Introduction | ▴Top |
Intestinal obstruction is a common surgical problem that surgeons face in usual clinical practice. About 15% of patients who were admitted to surgical department and complained of abdominal pain had small intestinal obstruction [1]. There are many causes of intestinal obstruction, which are either mechanical or functional (paralytic ileus). Each cause of intestinal obstruction needs different approach and management. Postoperative adhesion and hernia are the most common cause of small intestinal obstruction [2]. However, a relatively uncommon cause is a Meckel’s diverticulum. Although this diagnosis is primarily reported in the adolescent population, it should also be considered in adults. Meckel’s diverticulum is defined as due to the failure of complete obliteration of vitelline duct and this complication is more common in male. It is presented in 2-4% of the population and mostly it is discovered during surgical procedures. Most of Mackle’s diverticulum among adult is presented with bleeding [3, 4]. Our case report is presenting a diagnosis and management of recurrent intestinal obstruction due to Meckel’s diverticulum.
| Case Report | ▴Top |
A 25-years-old Saudi male patient who was medically free and had no prior abdominal surgery was referred from a peripheral hospital to our hospital (King Fasial Hospital Complex, Taif). He complained of abdominal pain, abdominal distension and vomiting that were precipitated by heavy meals, with no other associated symptoms. When he was admitted, he improved only after being kept nil per os (NPO) and given intravenous (IV) fluid without nasogastric tube (NGT) insertion. The patient suffered previously from recurrent episode of severe abdominal pain associated with abdominal distension and absolute constipation followed by vomiting. He was hospitalized several times for the same complains without any benefits. His adversity started when he was 10 years old. As stated by the patient, this episode is experienced on average of three times per year and improved with conservative management (NPO, NGT, and IV fluid) and sometime he had refused NGT and he would improve. He has refused laparotomy exploration several times.
At time of his recent presentation, he was vitally stable, afebrile; his abdomen was distended, tender with exaggerated bowl sound. No palpable masses were present. There were no hernia and no organomegaly. His complete blood count (CBC) profile and electrolytes were within normal levels. Abdominal X-ray showed multiple air fluid, distended small bowl and empty rectum, no air under diaphragm (Fig. 1). He was diagnosed initially with mechanical intestinal obstruction and was kept on NPO, IV fluid was given, NGT was refused and he improved. Computerized tomographic imaging of the abdomen with oral contrast was performed to establish the diagnosis and showed a distended small and large bowel, no mass, and no transition zone (Fig. 2). To identify the cause and to manage the patient properly, laparoscopy and laparotomy consent was taken. Initially, exploratory laparoscopy was done, but unfortunately the bowels were severally distended, for that reason we converted to laparotomy. Midline incision was done; the abdominal exploration showed free turbid fluid in the abdominal cavity. Multiple adhesions were released from ascending colon and distal small bowel until Meckel’s diverticulum was revealed with severe adhesion around, then bowel resection and side to side anastomosis was accomplished and washing with warm saline was done, then hemostasis was ensured (Fig. 3). Drain inserted and closure was done in layer. Meckel’s diverticulum was confirmed by a histology examination. He recovered without any complication and discharged after couple of days of hospitalization.
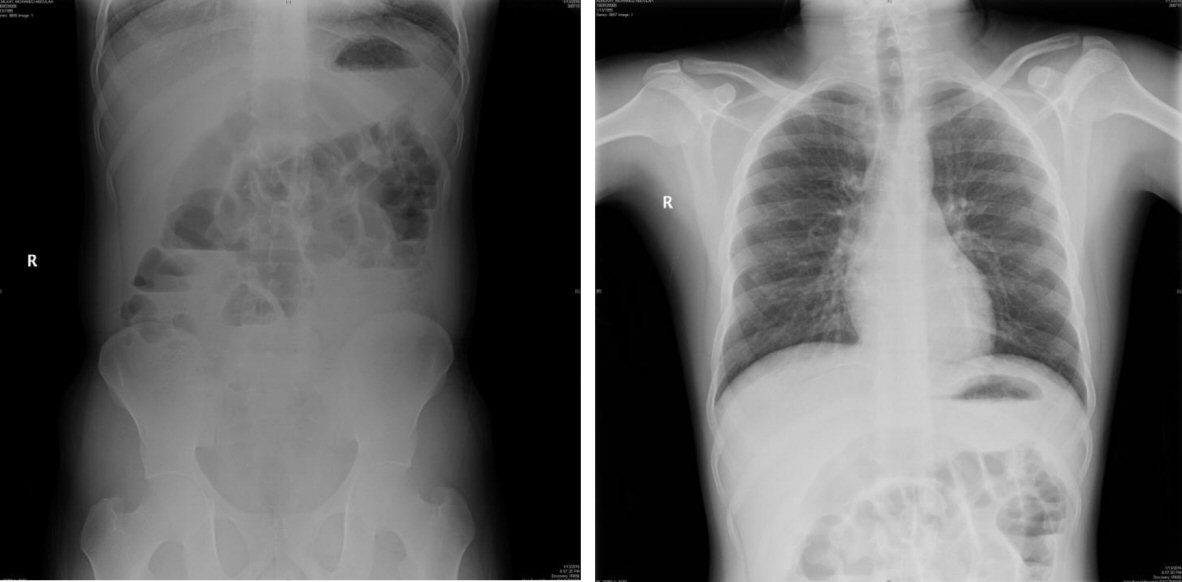 Click for large image | Figure 1. Upright abdominal X-ray (left) and chest X-ray (right) showed no air under diaphragm and distended bowel with multiple air fluid level. |
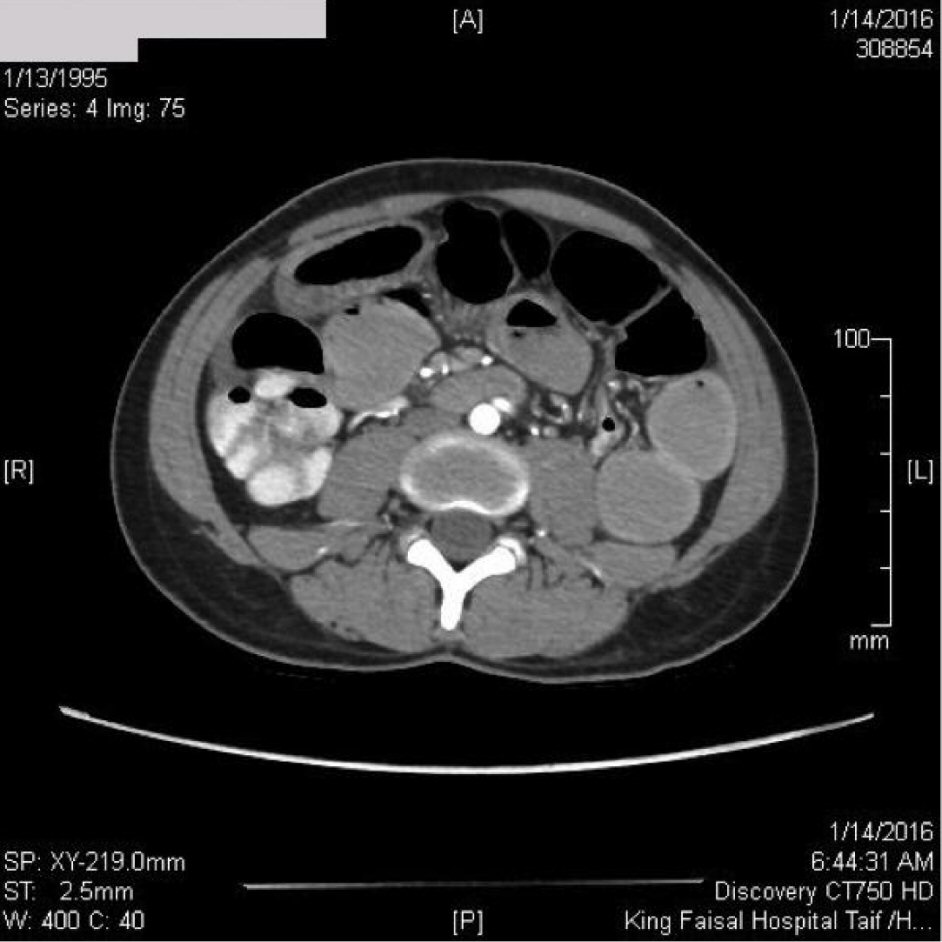 Click for large image | Figure 2. CT of abdomen with oral contrast showed a distended small and large bowel, no mass, and no transition zone. |
 Click for large image | Figure 3. Intraoperative photograph showed the 50 cm mass and 2 cm narrow base, amalgamated and adhesive ileum and ascending colon that making the obstruction. |
| Discussion | ▴Top |
Meckel’s diverticulum is presented in 2-4% of population due to failure of obliteration in the vitello-intestinal duct. It is the most common congenital disease of the gastrointestinal tract; however it is rare to occur in adult population. It is difficult to establish diagnosis preoperatively but computed tomography (CT), Technetium-99m and ultrasound are helpful for excluding other causes and determine some complications such as interception, volvulus and perforation [4]. Bleeding, intestinal obstruction and diverticulitis are the most frequent complications of Meckel’s diverticulum [3]. Most cases are asymptomatic but if intestinal obstruction is present, it is acute and due to adhesion around it, a Meckel’s diverticulum mass, volvulus, incarcerated hernia and interception may occur[3, 5]. In our case an adhesion was the cause of intestinal obstruction but it was strange that it was presented as partial intestinal obstruction, which is rare. Other complications in literature of Meckel’s diverticulum were reported as interception and lipoma can cause recurrent intestinal obstruction [6-8].
Conclusions
Complications of Meckel’s diverticula are uncommon in adult population. Intestinal obstruction, bleeding, and diverticulitis are most common presentations. Partial intestinal obstruction is rare presentation but it is documented.
Conflict of Interest
None.
Financial Support
None.
| References | ▴Top |
- Irvin TT. Abdominal pain: a surgical audit of 1190 emergency admissions. Br J Surg. 1989;76(11):1121-1125.
doi pubmed - Foster NM, McGory ML, Zingmond DS, Ko CY. Small bowel obstruction: a population-based appraisal. J Am Coll Surg. 2006;203(2):170-176.
doi pubmed - Park JJ, Wolff BG, Tollefson MK, Walsh EE, Larson DR. Meckel diverticulum: the Mayo Clinic experience with 1476 patients (1950-2002). Ann Surg. 2005;241(3):529-533.
doi pubmed - Sagar J, Kumar V, Shah DK. Meckel’s diverticulum: a systematic review. J R Soc Med. 2006;99(10):501-505.
doi pubmed - Dumper J, Mackenzie S, Mitchell P, Sutherland F, Quan ML, Mew D. Complications of Meckel’s diverticula in adults. Can J Surg. 2006;49(5):353-357.
pubmed - Jackson RH. Hemorrhagic ulcer of meckel’s diverticulum. Ann Surg. 1924;80(2):222-224.
doi pubmed - Karadeniz Cakmak G, Emre AU, Tascilar O, Bektas S, Ucan BH, Irkorucu O, Karakaya K, et al. Lipoma within inverted Meckel’s diverticulum as a cause of recurrent partial intestinal obstruction and hemorrhage: a case report and review of literature. World J Gastroenterol. 2007;13(7):1141-1143.
doi pubmed - Azar T, Berger DL. Adult intussusception. Ann Surg. 1997;226(2):134-138.
doi pubmed
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Current Surgery is published by Elmer Press Inc.